Cranial windows have become ubiquitously used throughout the fields of neuroscience, neural engineering, and biology to allow for direct visualization and imaging of the cortex in living animals1,2,3,4,5,6,7,8,9,10,11. The powerful combination of transgenic mice and multiphoton imaging has provided extremely valuable insights into circuit activity and other biological insights in the in vivo brain12,13,14,15,16,17,18. Miniature microscopes mounted on the skull have further extended these capabilities to enable recordings in awake, freely moving animals19. The process of creating a cranial window requires power-drilling to thin or completely remove the cranial bone to produce large enough craniotomies to secure a transparent piece of glass over the cortex20. Polydimethylsiloxane (PDMS) and other polymers have also been tested as cranial window materials9,21. Ultimately, the ideal cranial window is one that does not alter or interfere with normal endogenous activity underneath. However, it is commonly accepted that cranial window drilling aggravates underlying tissue, leading to damage to the brain, disruption of the environment, and effecting meninges to the point of occluding multiphoton imaging depth22. The resulting neuroinflammation has a wide array of effects ranging from permeability of the blood-brain barrier (BBB), to activation and recruitment of glial cells around the implant site23. Therefore, characterizing safer and more reproducible cranial window drilling methods is crucial for consistent imaging quality and reducing confounding factors.
While care is taken to minimize trauma to the underlying tissue, the act of drilling the bone has the potential to cause both thermal and mechanical perturbations to the brain24,25. Mechanical trauma from accidental drill penetration into the dura may further induce varying degrees of cortical injury24. In a study by Shoffstall et al.25, the heat from bone-drilling resulted in an increased BBB permeability, as indicated by the presence of Evans Blue (EB) dye in the brain parenchyma25. EB dye, injected intravenously, binds to circulating albumin in the bloodstream and therefore does not normally cross a healthy BBB in appreciable concentrations. As a result, EB dye is commonly used as a sensitive marker of BBB permeability26,27. While their study did not directly measure the impact of the BBB permeability on subsequent biological sequelae under study, prior studies have correlated BBB permeability to an increased neuroinflammatory response to chronically implanted microelectrodes and alterations in motor function28.
Depending on the goals of the study, the magnitude of thermal and mechanical damage may contribute a source of experimental error, negatively affecting the rigor and reproducibility of the study. There are dozens of cited methods for producing cranial windows, each using different drilling equipment, speeds, techniques, and users1,2,3,4,5,6,7,8,9,10,11. Shoffstall et al.25 reported that the observed variation in the heating outcomes was attributed to variability in the drill's applied force, feed rate, and angle of application, among other aspects that cannot be controlled for when drilling by hand25. There is a belief that automated drilling systems and other stereotaxic equipment can improve reproducibility and outcome consistency, but published method studies have not rigorously evaluated temperature or BBB permeability as one of the outcomes. Therefore, there is a need for more reproducible and consistently applied methods to produce cranial windows, as well as methods rigorously applied to assess the impact of cranial window drilling on underlying neural tissue.
The focus of this study is to determine and develop consistent and safe drilling methods for cranial windows. The size of the craniotomy for cranial window installation is significantly larger than standard craniotomies for brain implanted microelectrodes. Such craniotomies cannot be completed with a single burr hole when using standard equipment, thereby introducing more inter-surgeon technique variability when performed by hand20. Surgical drilling robots have been introduced to the field, but have not been widely adopted1,6,29. Automation of drilling offers control over variables contributing to observed trial-to-trial variation, suggesting that use of the equipment can reduce inter- and intra-surgeon effects. This is of particular interest given the added difficulty of the larger craniotomy needed for cranial window placement. While one could assume there to be clear benefits to the control provided by automating the drilling, there has been little assessment of the implementation of these equipment. Although visible lesions have not been observed5, the higher sensitivity test using EB is desired.
Here, BBB permeability is measured using a commercially available surgical drilling robot with corresponding software, which allows for programming of stereotaxic coordinates, craniotomy planning/mapping, and a selection of drilling styles ("point-by-point" vs "horizontal"), referring to the routed path of the drill bit. Initially, eight "seed" points are drilled (Figure 1A), outlining the cranial window. From here, the space in between the seeds is cut out using either the "point-by-point" or "horizontal" drill method. "Point-by-point" performs vertical pilot hole cuts (similar to a CNC drill press), while "horizontal" performs horizontal cuts along the circumference of the cranial window that outline the hole (similar to a CNC router). The result for both methods are a piece of skull that can be removed to reveal the cranial window. To isolate damage from drilling, the cranial window is not physically removed, so as to avoid any additional damage. A combination of EB dye coupled with fluorescent imaging is used to measure BBB permeability after performing craniotomies in mice, and an inserted thermocouple is used to directly measure temperature of the brain surface during drilling (Figure 1B,C). Previous observations indicated that pulsed drilling on/off with 2 s intervals was sufficient to mitigate drill heating25, and therefore is incorporated into the experimental approach for the surgical robot.
The intent of the presented work is to demonstrate methods of assessing thermal damage from craniotomy drilling. While the methods are presented in the context of automated drilling, such methods can be applied to manual drilling schemes as well. These methods can be used to validate the use of equipment and/or drilling schemes before adopting as a standard procedure.
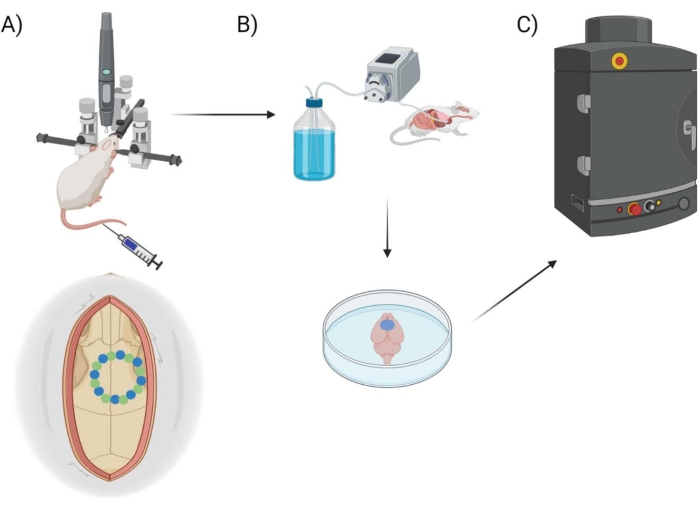
Figure 1: Experimental pipeline schematic. Schematic demonstrating the process animals underwent for EB quantification post-cranial window procedure. (A) Schematic setup of the mouse with the stereotaxic frame and surgical robot drill. An example cranial window is shown over the motor cortex with seed points (green) and edge points (blue). (B) The perfusion setup includes injecting 1x Phosphate Buffered Saline (PBS) throughout the animal to remove any blood, followed by extraction of the brain. (C) The brain is then put into the EB fluorescent imaging system chamber to conduct fluorescent imaging on the Evans Blue dye. Please click here to view a larger version of this figure.
Thermal evaluation
Potential for thermal damage was evaluated by measuring the change in temperature from baseline due to drilling using horizontal (Figure 2A), point-by-point (Figure 2B), and pulsed point-by-point (Figure 2C) methods. Figure 2D displays the experimental setup for obtaining thermal data. A sample size of N = 4 cranial windows was used for thermal evaluation. Horizontal and point-by-point use the same seed drilling schematic but vary on how the edge points are cut. Pulsed point-by-point employs a pulsed method for both seed and edge drilling portions. For the horizontal method, seed drilling showed a maximum temperature change of 16.66 °C ± 2.08 °C, while edge drilling showed 9.08 °C ± 0.37 °C. For the point-by-point method, seed drilling showed a maximum temperature change of 18.69 °C ± 1.75 °C, while edge drilling showed 8.53 °C ± 0.36 °C. For the pulsed point-by-point method, seed drilling showed a maximum temperature change of 6.90 °C ± 1.35 °C, while edge drilling showed 4.10 °C ± 0.51 °C. Both the horizontal and point-by-point drilling schemes show non-significant differences for thermal changes. However, changing to a pulsed point-by-point method resulted in significantly less heating (p < 0.05) of the brain than both horizontal and point-by-point drilling (Figure 2E,F). The duration of surgery was also recorded, as that may have an impact on animal survivability for live surgeries. For both automated methods, the seed drilling took 360 s on average. Horizontal edge drilling took 300 s, while point-by-point edge drilling took 200 s. The pulsed method took the longest, with seed and edge drilling taking approximately 500 s each. Nevertheless, these differences are not large enough to warrant any consideration as surgeries can commonly last over 2-3 h.
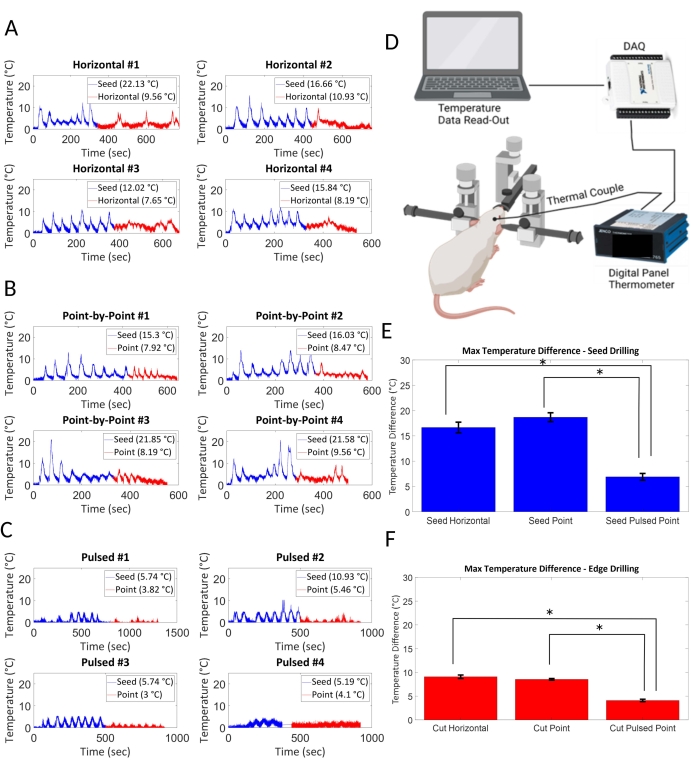
Figure 2: Thermal evaluation. Potential for thermal damage was evaluated based on maximum temperature changes in the brain as a result of drilling methods. (A) Horizontal drilling and (B) point-by-point drilling generated similar amounts of heat, whereas (C) a pulsed 2 s on, 2 s off point-by-point method showed minimal heating. (E) Seed drilling and (F) edge drilling resulted in significantly less thermal change in the pulsed point-by-point method of drilling (p < 0.05, N = 4 per condition). (D) The thermocouple is placed underneath the skull of the mouse cadaver where the drilling is done. Data is acquired through a DAQ and fed into a computer for analysis. Please click here to view a larger version of this figure.
Vascular damage
Figure 3 indicates the relationship between drilling scheme and vascular damage. Table 1 indicates the p-value for each drilling scheme following statistical analysis as indicated in step 10. A sample size of N = 4 per group was used for EB dye evaluation. The presence of a higher amount of EB is a direct indicator of damage to the BBB, of which the point-by-point, horizontal, and pulsed drilling methods are significantly larger than that of the control (all with p = 0.043; Table 1). The point-by point method does not show any significant difference in terms of EB presence compared to the horizontal drilling (p = 0.411). Both these schemes employed the auto-stop function to prevent drilling into the brain; however, this auto-stop function often failed to prevent damage. This failure of auto-stop in the shared seed drilling portion could have caused unknown excess damage, complicating differentiation between the techniques. Therefore, a pairwise comparison to a pulsed point-by-point method without auto-stop was performed to evaluate the other two methods without incorporating auto-stop. There was no significant difference when pulsed point-by-point was compared to point-by-point (p = 0.486), whereas the pulsed point-by-point method had significantly less EB presence than the horizontal method (p = 0.043). Non-significance between pulsed point-by-point and point-by-point methods may be attributed to the large variation in point-by-point drilling (Figure 4).
Figure 3 shows representative images of both horizontal (Figure 3C) and point-by-point (Figure 3D) drilling with proper auto-stop features. Visually, and through EB fluorescent imaging, drilling via point-by-point and horizontal cutting was seen to be damaging to the vasculature in the brain in comparison to control groups (Figure 3A,B). The pulsed point-by-point method (Figure 3E) had less localized damage at the seed and edge point, but still had visible EB presence within the cranial window.
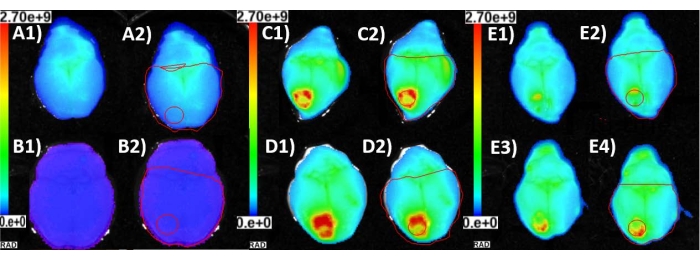
Figure 3: Vascular damage. EB fluorescence images of explanted brains (1) and corresponding ROIs (2) utilized to determine the mean radiance of the area affected by cranial window craniotomy. (A) The mouse was injected with EB with no cranial window surgery to acquire baseline background EB presence in the brain vasculature. (B) The mouse was injected with saline only and a cranial window craniotomy was performed. This established that the mean radiance being measured was credited to the EB accumulation due to leaky blood vessels and vascular trauma near the site of the cranial window. (C) The mouse was injected with EB and the cranial window was created by the horizontal method of automatic drilling. (D) The mouse was injected with EB and the cranial window was created by the point-by-point method of automatic drilling. (E) Two representative images of cranial window produced with the point-by-point pulsed method of drilling after the mice (n = 2) were injected with EB. Please click here to view a larger version of this figure.
Visual inspection of damage
Visually inspecting the brains shows physical damage to the surface of the brain (Figure 4). The panels A–D demonstrate the EB presence of the horizontal drilling, panels E-H the point-by-point method, and panels I-L are the pulsed point-by-point method. "Point-by-point" performs vertical pilot hole cuts while "horizontal" performs horizontal cuts along the circumference of the cranial window that outline the hole. The "pulsed point-by-point" employs the same methods as the point-by-point without the use of the auto-stop feature, and depends on the user stopping the drilling at set increments of depth. Although a method has been found that will minimize the amount of thermal damage to the brain, there is still the issue of mechanical damage from the drill. Ideally, an auto-stop feature that detects CSF and stops drilling before damaging brain tissue would work here, but did not seem to work consistently. Even with extreme care taken in pulsed manual drilling, there was still visual damage on the brain. This could be the result of two factors: 1) the lack of control and feel that comes with hand drilling and 2) the separation depth between the skull and the brain for a small animal such as a mouse. Hand drilling may offer a more controlled method for getting through the skull without damaging the brain with enough practice and expertise. However, there is much higher skill and training needed compared to a plug-and-play robot, which would allow for several "surgeons" to contribute to the same study-not a common practice in the intracortical microelectrode field. With mice, the distance between the brain and skull is extremely thin, so even the slightest over-drill of 10 µm can lead to mechanical damage to the brain.
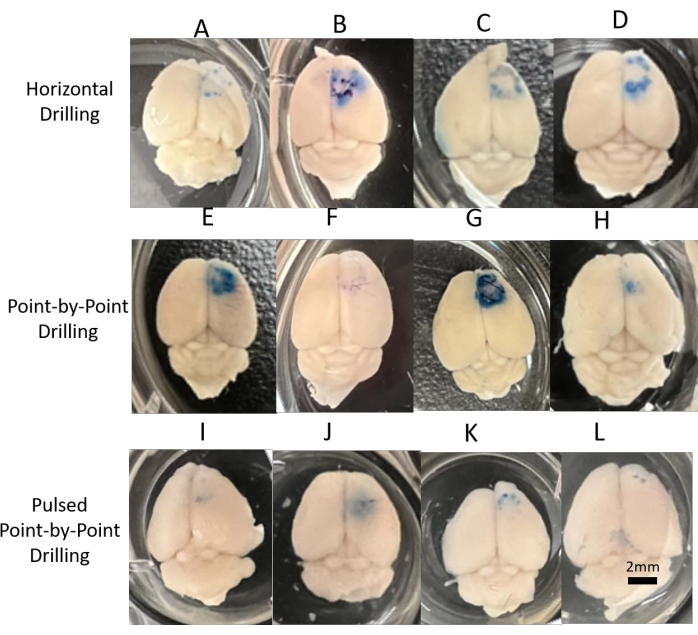
Figure 4: Visual inspection of damage. Digital images of all brains acquired for visual inspection and representation for each of the three drilling methods. (A–D) Horizontal consistently showed damage around the cranial window, whether from mechanical or thermal damage. (E–H) Point-by-point showed considerable variance in results, indicating a less reliable method for drilling. (I–L) Pulsed point-by-point was more consistent and showed less visual damage than the other methods, matching the differences in EB fluorescent analysis and thermocouple results. Scale bar = 2 mm. Please click here to view a larger version of this figure.
| Horizontal | Point | Pulsed | Control | |
| Horizontal | – | 0.411 | 0.043* | 0.043* |
| Point | 0.411 | – | 0.486 | 0.043* |
| Pulsed | 0.043* | 0.486 | – | 0.043* |
Table 1: Statistical analysis of EB fluorescent imaging results. Results from the EB fluorescent imaging system for different drilling techniques were analyzed using a Kruskal-Wallis rank sum test with Benjamin-Hochberg correction followed by pairwise comparisons using the Wilcoxon rank sum exact test (N = 4 per group). Significant differences between groups are indicated with an asterisk *.
