The protocol presented here is highly reproducible and resulted in a third-degree, full-thickness burn injury in rats. The burn wound appears waxy white after burn induction (Figure 2B). The color of the burn injury changed from white to brown over the course of 72 h post burn (Figure 2B–E).
Histological analysis confirmed a full-thickness burn (depth >2.61 mm at 24 h post burn; Figure 3B). Compared to intact non-burn skin, skin samples from burn animals showed evidence of injury across all layers at 24, 48, and 72 h post burn injury (Figure 3). Additionally, histological analysis showed complete destruction of the epidermal layer and damage to the full thickness of the dermis with involvement of subcutaneous fat and skeletal muscle (Figure 3B).
To evaluate bacterial clearance, various tissues were harvested at 24, 48, and 72 h following infection with P. aeruginosa and S. aureus. Bacteria were recovered from the infection site for all burn injury rats (Figure 4A,B). Furthermore, the number of bacteria recovered from the skin of burn rats was less than the initial inoculum for P. aeruginosa at 24 h post infection, whereas tissue samples obtained at 48 and 72 h post burn and infection showed an increase in the bacterial burden (Figure 4A). In contrast, a 2 log10 increase was observed at all time-points for S. aureus in the skin compared to the initial inoculum (Figure 4B). This suggests that S. aureus was able to establish infection because of its active replication in the tissues and not solely because of immunosuppression induced by the burn injury.
Different layers of the skin (i.e., subcutaneous tissue, muscles, and distal organs) were also analyzed to examine bacterial dissemination. The subcutaneous tissue and muscles showed a higher bacterial load than the lung and spleen. Taken together, these data show that burn rats develop a systemic infection 24 h or 48 h following wound inoculation with P. aeruginosa (Figure 4A) or S. aureus, respectively (Figure 4B). Complete blood counts were also obtained using a hematology analyzer (see the Table of Materials) at baseline and 72 h post burn injury. Total white blood cell counts decreased over time, indicating immune suppression. Neutrophil counts declined after burn but increased following infection at 72 h compared to the baseline (Table 1). However, increases in red blood cell and platelet counts were observed after burn and infection, indicating systemic inflammation.
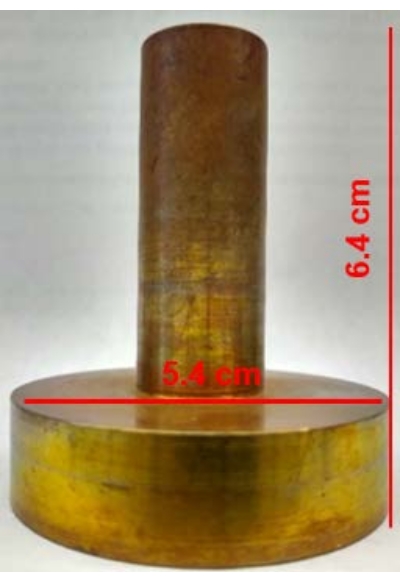
Figure 1: Copper rod employed to inflict burn induction. The weight of the custom-made rod is 420 g with a 5.4 cm diameter and 6.4 cm height. Please click here to view a larger version of this figure.
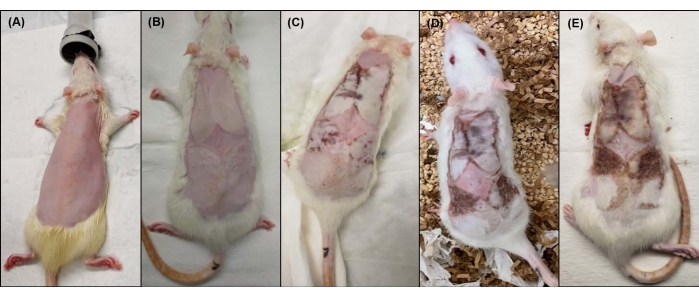
Figure 2: Macroscopic view of the rat dorsal side before and after burn induction. (A) Rat dorsum after shaving, (B) immediately after burn injury, (C) 24 h post burn, (D) 48 h post burn, and (E) 72 h post burn. Please click here to view a larger version of this figure.
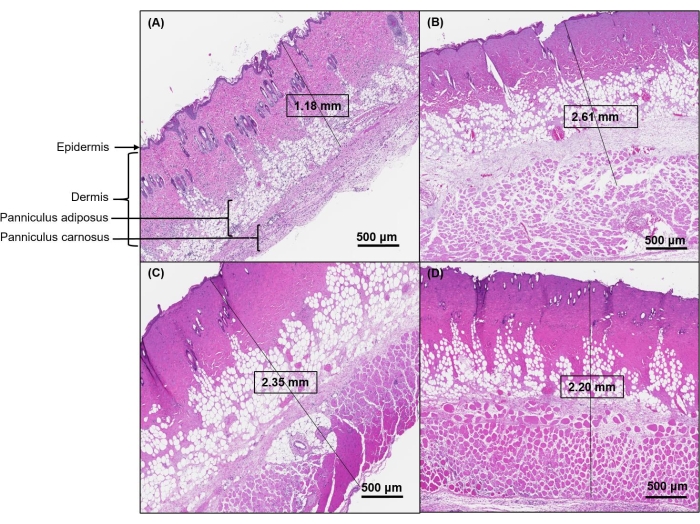
Figure 3: Representative images of H&E-stained cross-sections for each level of burn severity. (A) The histology of sham rat skin shows a clear distinction between epidermis, dermis, and subcutaneous tissue layers. (B) Skin histology 24 h post burn shows attenuated epidermis with coagulative damage to the full thickness of the dermis and the subcutaneous tissue with a maximum burn depth of >2.61 mm. (C) At 48 h post burn, the maximum burn depth was 2.35 mm, and (D) at 72 h post burn, the maximum burn depth was 2.20 mm. Images were scanned at 40x magnification. Scale bars = 500 μm (A–D). Abbreviation: H&E = hematoxylin and eosin. Please click here to view a larger version of this figure.
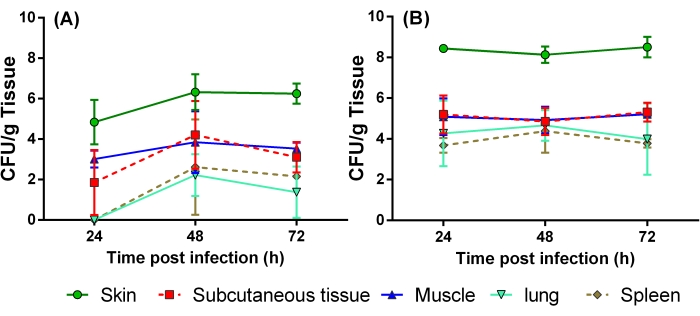
Figure 4: Quantification of bacterial load in different organs after infection of burn wound. Rats were infected with 6 log CFU of the bacteria via subcutaneous injections 15 min after the burn injury. Skin, subcutaneous tissue, muscle, lung, and spleen were collected at 24, 48, and 72 h post infection to determine the progression of systemic disease. Three rats were used at each time point.(A) Pseudomonas aeruginosa PA01, (B) Staphylococcus aureus ATCC25923. Abbreviation: CFU = colony-forming units. Please click here to view a larger version of this figure.
| Cell type | Baseline (average ± SD) | 72 h Un-infected (average ± SD) | 72 h-Infected (average ± SD) |
| White Blood Cells (109/L) | 16.9 ± 4.9 | 7.1 ± 2.0 | 6.50 ± 5.5 |
| Neutrophil (109/L); (%) | 4.0 ± 1.1; (24.3 ± 2.8) | 1.4 ± 0.4; (20.2 ± 5.7) | 1.88 ± 1.0; (35.0 ± 12.4) |
| Lymphocytes (109/L); (%) | 11.6 ± 4.1; (68.5 ± 1.7) | 4.8 ± 1.7; (66.5 ± 7.6) | 3.54 ± 3.9; (46.4 ± 17.0) |
| Monocytes (109/L); (%) | 0.9 ± 0.3; (5.4 ± 1.5) | 0.8 ± 0.2; (11.5 ± 1.6) | 1.0 ± 0.6; (17.3 ± 5.5) |
| Red blood cells (1012/L) | 7.5 ± 0.3 | 7.1 ± 0.8 | 10.0 ± 1.1 |
| Hemoglobin (g/dL) | 14.3 ± 0.7 | 13.4 ± 1.0 | 18.6 ± 2.0 |
| Platelets (109/L) | 723.3 ± 353.1 | 942.7 ± 43.1 | 1359.0 ± 228.5 |
| HCT (%) | 45.6 ± 3.0 | 39.9 ± 3.7 | 55.7 ± 8.2 |
Table 1: Hematology parameters before and after burn infliction and infection. Abbreviation: HCT = hematocrit.
Supplementary File 1: Steps to analyze H&E images in Aperio ImageScope. Abbreviation: H&E = hematoxylin and eosin. Please click here to download this File.
