Full-Endoscopic Isolation Zone Technique for the Treatment of Lumbar Disc Herniation
Summary
Here, we present a protocol for the "isolation zone" technique in the treatment of lumbar disc herniation (LDH) under full-endoscopic spine surgery (FESS), including intervertebral foramen formation, targeted catheterization, nucleus pulposus resection, and annulus fibrosus formation, which together completely block the pain from the nerve conduction pathway.
Abstract
Lumbar disc herniation (LDH) is a type of serious sinus or sciatic nerve dysfunction caused by nucleus pulposus protrusion and annulus fibrosus tears. Its clinical symptoms often include severe low back pain, limited lumbar movement, sciatic nerve pain in the lower limbs, and even cauda equina syndrome. The common treatment for LDH is a conservative treatment scheme involving medicine, rest, and physical therapy. However, if the conservative treatment scheme is ineffective, a surgical treatment approach is adopted. Traditional open lumbar surgery has some disadvantages, including the potential for severe surgical trauma, severe blood loss during the operation, instability of the lumbar spine, and loss of the lumbar motor unit. Among the minimally invasive surgical schemes, full-endoscopic spine surgery (FESS) is undoubtedly the most appropriate and has the advantages of minimal trauma, high safety, quick postoperative recovery, and the retention of the stable structure and the motor unit of the lumbar spine. However, simultaneously, incomplete removal of the nucleus pulposus and residual nerve dysfunction after surgery can occur. To avoid these shortcomings, we studied a specific spinal endoscopy technique, the “isolation zone” surgical strategy, which can effectively block the pain from the nerve conduction pathway by completely relieving the nerve compression and nerve dysfunction through the orderly treatment of the protruding nucleus pulposus, the fissure of the annulus fibrosus, the sinus nerve, and the surrounding inflammatory soft tissues.
Introduction
LDH is a common degenerative disease of the spine. LDH is accompanied by multifactorial changes, such as degeneration of the intervertebral disc and the surrounding structures. The interaction between multifactorial degeneration and the nervous system causes pain1. The pain of this disease manifests as low back pain and leg pain, and sometimes LDH can be related to an inability to maintain the same posture or sensory-motor disorder of the lower limbs2. The severe clinical symptoms of LDH bring great pain to the patients and represent a serious medical and social problem3,4. For patients with obvious herniated intervertebral discs or a torn annulus fibrosus, traditional conservative treatments, including drug therapy, physical therapy, and rest, cannot effectively solve their problem5. Lumbar fusion surgery is usually used to treat patients with LDH for whom conservative treatment is ineffective6. However, this surgery has a high economic cost and causes large surgical trauma and destruction of the stable structure of the spine; additionally, the postoperative improvement in low back pain, sensory-motor disturbance of the lower limbs, and lumbar motion function, etc., is sometimes unsatisfactory7. The development of FESS has not only improved the curative effects of lumbar surgery but also reduced the cost and risk of surgery8,9. However, if the nucleus pulposus is not completely removed during endoscopic surgery and the treatment of the pain-inducing factors is not comprehensive, the patient will have low back pain, dysesthesia in the lower extremities, and other adverse reactions after surgery10,11,12,13.
To avoid inadequate removal of the nucleus pulposus during endoscopic surgery and the inadequate relief of postoperative neurological dysfunction, our research team applied a modified spinal endoscopic "isolation zone" technique. The "isolation zone" technology aims to block the pain transmission pathway of the sinus vertebra nerve and sciatic nerve by removing the herniated intervertebral disc, ruptured annulus fibrosus, and hyperplastic inflammatory tissue. In addition, pathogenic inflammatory mediators on the surface of the disc and intraspinal canal are removed13. The "isolation zone" technique can fully decompress the unilateral compressed spinal nerves. This technical strategy is more minimally invasive and effective than traditional surgical methods.
Protocol
The protocol follows the guidelines of the Ethics Committee of Cangzhou Central Hospital (No.: 20210205). Informed consent was obtained from the patients to include them, and the data were generated as part of this study.
1. Pre-operative preparation
- Select patients according to the following inclusion and exclusion criteria.
- Follow the inclusion criteria mentioned below:
- Include patients with lower waist pain caused by long-term sitting, standing, walking, and waist activities, with or without typical sciatic nerve pain.
- Include patients with preoperative X-ray, CT, MRI, or other imaging data showing single-segment intervertebral disc herniation or an annulus fibrosus tear, an intervertebral space that does not collapse, and no bony spinal stenosis.
- Include patients with a physical examination showing obvious neurological dysfunction of the lower limbs and a positive straight leg elevation test.
- Include patients with ineffective systematic conservative treatment for at least 6 weeks and clinical symptoms seriously affecting their work and life.
- Include patients with low back pain without lower limb nerve pain. For these patients, perform a selective nerve block by using a mixture of low-concentration lidocaine and triamcinolone acetonide through the intervertebral foramen. This decreases the visual analog scale (VAS) of low back pain by more than 50% within 48 h.
- Follow the exclusion criteria mentioned below:
- Exclude patients with lumbar instability or spondylolisthesis.
- Exclude patients with lumbar intraspinal tumors or spinal cord tumors.
- Exclude patients with ligamentum flavum hypertrophy or contralateral recess stenosis.
- Exclude patients with mental disorders.
- Exclude patients with coagulation dysfunction.
- Exclude patients who are unwilling to undergo surgery.
NOTE: The anesthesia mode was local infiltration anesthesia, and the surgical position was lateral. The procedures were performed on patients in the side-lying position under the guidance of a G-arm or C-arm X-ray machine.
- Follow the inclusion criteria mentioned below:
2. Anesthesia and lesion exposure
- Administer local anesthesia to all the patients (15 mL of 2% lidocaine + 10 mL of 1% ropivacaine + 45 mL of 0.9% saline).
NOTE: The anesthesia level is the skin, the superficial subcutaneous fascia, the thoracolumbar fascia, the facet joint, and the surface of the annulus fibrosus of the intervertebral disc. - Use an 18 G puncture needle to puncture the bottom of the articular process. Ensure that the tip of the puncture needle is located at the inner edge of the articular process in the anteroposterior X-ray and at the center of the intervertebral space or the upper edge of the distal vertebral body in the lateral X-ray.
- Place a thin guide wire through an 18 G puncture needle, and make a 7 mm skin incision. Place soft tissue expansion catheters with different diameters through the guide wire, and then pace the Tom Shidi locator along the guide wire (Figure 1A).
- Fix the tip of the Tom Shidi locator on the tip of the superior articular process, pointed toward the target of the herniated disc, and gently hammer it to make it pass through the articular process bone. Adjust the depth of the Tom Shidi locator entering the spinal canal according to the position of the herniated disc (Figure 1C, D).
- Remove the Tom Shidi locator, replace the guide wire, and use bone drills with different diameters to operate along the guide wire (Figure 1B), which is used to grind off part of the facet joints for intervertebral aminoplasty (Figure 1E, F).
NOTE: The high-intensity zone of the L4/5 segment intervertebral disc annulus fibrosus and the nucleus pulposus protrusion can be seen in the preoperative lumbar MRI (Figure 2A, B). - After the intervertebral foramen is formed by a bone drill (4 mm, 5 mm, 6 mm, 7 mm, and 8 mm diameter), insert the guide rod along the guide wire. Place the endoscope working channel along the guide rod, and confirm that the working channel has reached the target point by intraoperative fluoroscopy again (Figure 2C, D).
3. "Isolation zone" technique of spinal endoscopy
- Percutaneously and transforaminally place a 7.5 mm diameter spinal endoscope with a 3.7 mm diameter working channel at the lumbar disc herniation at the appropriate level to explore and clean the ligaments and the residual bone fragments in the intervertebral foramen area, the soft tissues in the spinal canal, and the protruding lumbar intervertebral disc.
- Remove the proliferated, inflamed, and red soft tissues scattered in the vertebral canal with microscopic surgical instruments. Use nucleus pulposus forceps to explore the torn area of the annulus fibrosus, and remove the severely degenerated and inelastic tissue.
- Remove the ruptured part of the annulus fibrosus and the protruding nucleus pulposus using miniature surgical forceps. Use flexible bipolar radiofrequency to coagulate the annulus fibrosus and the nucleus pulposus to stop the bleeding and shrink and denervate them.
- When there is enough space around the nerve root and the dural sac during the operation, use flexible bipolar radiofrequency to perform an annuloplasty and nucleoplasty on the residual annulus fibrosus and nucleus pulposus, respectively.
- Explore the nerve root with a miniature probe hook to ensure that it has sufficient space and spontaneous pulsation (Figure 2E). Remove the endoscope and its working channel, and suture the skin with a 4-0 nonabsorbent surgical thread suture.
4. Intraoperative drug application
- During the operation, always use the endoscopic instrument under continuous irrigation with normal saline. According to the condition of the patient, choose appropriate intravenous hemostatic drugs (e.g., preoperative intravenous drip of 1 g of tranexamic acid) or analgesic drugs (e.g., preoperative intravenous drip of 100 mg of flurbiprofen axetil).
- If the patient is sensitive to pain or has severe nerve stimulation during the operation, ask the anesthesiologist for help with the application of sedative and analgesic drugs during the operation.
- After the operation, suture the skin and superficial fascia at the incision of the spinal endoscope without placing a drainage tube. Inject ropivacaine around the incision to relieve pain and discomfort around the incision.
5. Post-operative care
- Provide postoperative analgesia with oral or intravenous drugs (for example, oral diclofenac sodium sustained-release tablets at 75 mg/day or intravenous flurbiprofen axetil at 100 mg/day) for 3-5 days, neurotrophic drugs (oral mecobalamin tablets, 5 mg each time, three times per day) for 6 weeks, and the appropriate symptomatic treatment.
- On the first day after the operation, advise the patient to get out of bed and move around while wearing a lumbar orthosis. Under the protection of the lumbar orthosis, advise the patient to exercise their limbs. Instruct the patient to carry out functional exercises of the lumbar back muscles, straight leg lifting (SLR) exercises, and functional exercise plans every day.
Representative Results
FESS with the "isolation zone" strategy was adopted in this study to treat LDH, and this method effectively relieved the patients' low back pain and/or sciatic nerve pain. For all the patients who underwent surgery under local anesthesia, the operation did not have to be interrupted because of unbearable pain. The VAS score, ODI index, and the excellent and good rates of the modified MacNab criteria from the previous study are shown in Table 1.
The MRI re-examination of the lumbar spine after the operation showed that the herniated intervertebral disc disappeared, and the tear of the annulus fibrosus disappeared and healed well, forming an "isolation zone" on the ventral side of the dura mater and nerve root (Figure 2F-I).
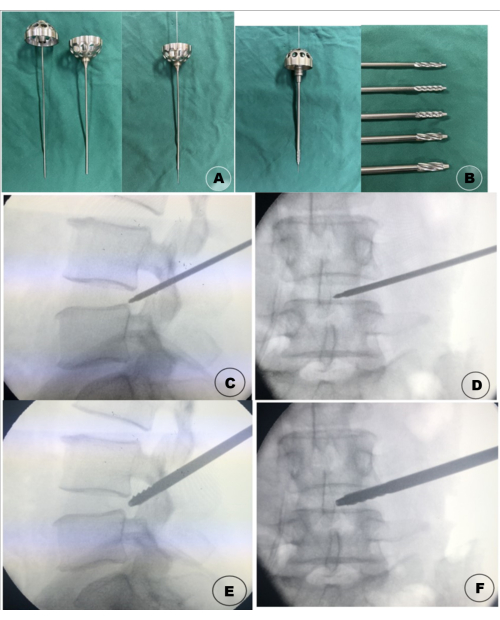
Figure 1: Surgical instruments and intraoperative diagrams of the intervertebral foramen plasty. (A) The Tom Shidi locator combined with the guide wire. (B) The bone drill combined with the guide wire. (C) Intraoperative lateral X-ray of the Tom Shidi locator; (D) Intraoperative AP X-ray of the Tom Shidi locator; (E) Intraoperative lateral X-ray of the bone drill. (F) Intraoperative AP X-ray of the bone drill. Please click here to view a larger version of this figure.
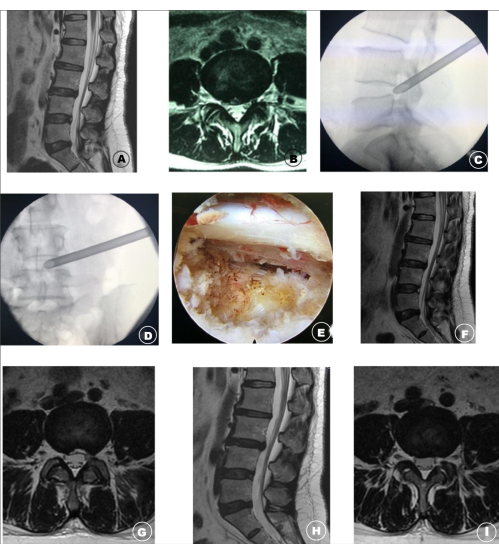
Figure 2: Image data of LDH patients before, during, and after the operation. (A,B) The high-intensity zone of the L4/5 segment intervertebral disc annulus fibrosus and the nucleus pulposus protrusion can be seen in the preoperative lumbar MRI. (C,D) The working channel of the spinal endoscopy during the operation. (E) Intraoperative images showing the "isolation area" formed in the nerve root and ventral dura mater after endoscopic decompression. (F,G) At 1 week after the operation, the lumbar MRI was rechecked, and the signal of the fibrillar ring tear disappeared; the range of ventral decompression of the dura mater was sufficient. (H,I) The lumbar MRI was re-examined 10 months after the operation, and the fibrous ring tear disappeared; the surgical scope of the "isolation area" healed well. This figure has been modified with permission from Wang et al.14. Please click here to view a larger version of this figure.
| Patients (n = 45) | |
| VAS score | |
| Pre-operation | 6.95 ± 1.02 |
| 1 month after operation | 2.64 ± 0.71 |
| 3 months after operation | 1.80 ± 0.54 |
| 6 months after operation | 1.42 ± 0.50 |
| 12 months after operation | 1.27 ± 0.45 |
| ODI | |
| Pre-operation | 72.84 ± 5.95 |
| 1 month after operation | 35.1 ± 5.30 |
| 3 months after operation | 25.22 ± 4.85 |
| 6 months after operation | 16.78 ± 4.63 |
| 12 months after operation | 10.91 ± 2.36 |
| Treatment effect | |
| Excellent | 24 (53.3%) |
| Good | 13 (28.9%) |
| Fair | 8 (17.8%) |
Table 1: VAS score and ODI index. This table has been modified with permission from Wang et al.14.
Discussion
LDH is a degenerative disease of the spine that seriously affects daily life and work. The main clinical manifestations are low back pain and sciatic nerve pain. Extreme waist movements, fixed posture, and physical labor can aggravate the symptoms4,15. If conservative treatment cannot alleviate the clinical symptoms, minimally invasive methods are used to treat patients with LDH. Momenzadeh et al. used percutaneous laser disc decompression (PLDD) to treat 30 patients with LDH, and the results showed that the VAS and ODI scores of the patients were decreased after percutaneous laser discectomy16. Zhang et al. treated 307 patients with lumbar disc herniation or lumbar spinal stenosis by endoscopy or microscopy, which effectively relieved acute nerve root symptoms; additionally, there were no differences in the ODI scores and VAS scores at the end of follow-up17. In another study, 24 patients with DLBP were treated with the outside-in technique of percutaneous spinal endoscopy for annulus fibrosus tears18. At the 12 month follow-up, the average VAS score decreased from 6.83 ± 0.87 before the operation to 1.62 ± 0.7718. Therefore, with all these minimally invasive methods, the clinical symptoms are obviously improved. However, most studies focus on minimally invasive surgical tools and surgical approaches, and there are few studies on the specific operation steps and treatment scope19,20.
At present, it is considered that the pathogenesis of LDH mainly involves nucleus pulposus protrusion and an annulus fibrosus tear caused by lumbar degeneration, pain caused by inflammatory factors and produced by pain receptors of the sinus nerve when it is tightly covered by the intervertebral disc, and radiation pain of the lower limbs caused by sciatic nerve compression and ischemia edema21. In particular, under the action of oppressive stimulation of inflammatory mediators in the herniated nucleus pulposus, hyperplastic inflammatory nerve endings can appear at the rupture of the annulus fibrosus and in the nucleus pulposus, thus inducing low back pain22. The herniated disc squeezes the ligaments in the spinal canal, nerve root, and dura mater, which causes continuous stimulation of the inflammatory mediators in the annulus fibrosus tear and, thus, synergistic neurological dysfunction. The continuous stimulation of inflammatory mediators leads to the formation of a pannus and new nociceptive nerve fibers near the annulus fibrosus and, gradually, chronic and scattered inflammatory lesions, which aggravate the pain stimulation23. If the herniated nucleus pulposus, annulus fibrosus, and surrounding nonbacterial inflammatory tissues are not thoroughly removed during endoscopic surgery, there will often be postoperative residual low back pain or sciatic nerve stimulation of the lower limbs.
Compared with traditional endoscopic discectomy, the "isolation zone" technique for the treatment of lumbar disc herniation has more complicated endoscopic operation requirements and requires more surgical details. The key points of the "isolation zone" surgical strategy are the accurate location and safe anatomical access. The range of endoscopic exploration and operation needs to reach the posterior inferior edge of the upper vertebral body at the proximal end, the posterior superior edge of the lower vertebral body at the distal end, and the longitudinal fibers of the posterior longitudinal ligament inward. The protruding nucleus pulposus must be removed as completely as possible, the hyperplastic inflammatory tissue in the spinal canal must be removed, the intervertebral disc that is protruding and compressing the spinal nerve must be removed, the sinus plexus must be blocked with radio frequency, the torn part of the annulus fibrosus should be removed, shrunk, and denervated, the periphery of the posterior longitudinal ligament should be denervated, and an "isolation zone" should be formed around the nerve root and dura mater to block the conduction of inflammatory factors and pain by the nerve fibers.
In this study, the isolation zone technology of FESS used has the following advantages in treating LDH. 1) The application of selective nerve block through the intervertebral foramen before the endoscopic surgery allows the surgeon to accurately find the involved segment of the LDH, especially for patients with complicated symptoms and unclear involved segments, and selective nerve block can avoid disc injury and false positives caused by the injection of contrast agent into the disc. 2) The FESS isolation zone technique has little influence on the stable structure of the lumbar spine and allows the motor unit of the spine to be retained. It is obviously superior to traditional fusion surgery in preventing the postoperative degeneration of adjacent segments. 3) Under local anesthesia, patients can correctly report on the neurological status of the lower limbs during the operation. The incidence of nerve injury is low, patients can exercise soon after the operation, and lumbar function can recover quickly after surgery. 4) The isolation belt technology can be used to comprehensively treat all the pathogenic factors of LDH, with few residual symptoms after surgery and satisfactory treatment effects.
The "isolation zone" technique of the FESS has several limitations. As the range of treatment under endoscopy is large, there are certain requirements for the accuracy of the placement of the endoscope working channel. In addition, this technique requires the identification and thorough cleaning of various pathogenic factors in the involved segment of the lumbar disc herniation. This technique also requires sufficient intervertebral foramen formation because it is sometimes necessary to constantly move the direction of the endoscope to achieve sufficient surgical vision. If the ventral facet of the facet joint is not sufficiently removed or the intervertebral foraminoplasty is not sufficient, the scope of the endoscope treatment will often be limited, so there are certain requirements for the operator's endoscopic operation level. If the operator wants to fully understand and master the "isolation zone" technique, the learning curve is steep.
The FESS "isolation zone" technique is a very significant technique in the treatment of LDH. Due to its comprehensive treatment strategy and effective blocking pain from the nerve conduction pathway, this technique can also play an important role in the treatment of lumbar spinal stenosis, lumbar spondylolisthesis, and discogenic low back pain in the future.
Divulgations
The authors have nothing to disclose.
Acknowledgements
None.
Materials
| 18 G puncture needle | tong lu | KB401.061 | |
| 3.7 mm spinal endoscope | joimax | FS6342181C | |
| 4-0 nonabsorbent surgical suture | Johnson & Johnson | WB761 | |
| 7.5 mm working channel | maxmore | 1001-ES04 | |
| Bone drill | maxmore | 1001-BD(001-005) | 4 mm, 5 mm, 6 mm, 7 mm, 8 mm diameter |
| C-arm X-ray machine | GE | OEC one | |
| Catheters | maxmore | 1001-DC 001 | |
| Expansion guide rod | maxmore | 1001-DC 002 | |
| Flexible bipolar radiofrequency | tian song | G8002.2 | |
| Guide wire | maxmore | 1001-GW 003 | 1mm diameter |
| Nucleus pulposus forceps | maxmore | 1001-EF 001 003 | 0°and 15° |
| Tom Shidi locator | maxmore | 1001-TS 001 |
References
- Fujii, K., et al. Discogenic back pain: Literature review of definition, diagnosis, and treatment. JBMR Plus. 3 (5), 10180 (2019).
- Urits, I., et al. Low back pain, a comprehensive review: Pathophysiology, diagnosis, and treatment. Current Pain and Headache Reports. 23 (3), 23 (2019).
- Geurts, J. W., Willems, P. C., Kallewaard, J. W., van Kleef, M., Dirksen, C. The impact of chronic discogenic low back pain: Costs and patients’ burden. Pain Research & Management. 2018, 4696180 (2018).
- Kallewaard, J. W., et al. Discogenic low back pain. Pain Practice. 10 (6), 560-579 (2010).
- Peng, B., et al. Prospective clinical study on natural history of discogenic low back pain at 4 years of follow-up. Pain Physician. 15 (6), 525-532 (2012).
- Bydon, M., et al. Lumbar fusion versus nonoperative management for treatment of discogenic low back pain: A systematic review and meta-analysis of randomized controlled trials. Journal of Spinal Disorders & Techniques. 27 (5), 297-304 (2014).
- Zhao, L., Manchikanti, L., Kaye, A. D., Abd-Elsayed, A. Treatment of discogenic low back pain: current treatment strategies and future options-a literature review. Current Pain and Headache Reports. 23 (11), 86 (2019).
- Yagi, K., et al. Advantages of revision transforaminal full-endoscopic spine surgery in patients who have previously undergone posterior spine surgery. Journal of Neurological Surgery, Part A: Central European Neurosurgery. , (2022).
- Okada, R., et al. Preoperative planning using three-dimensional printing for full-endoscopic spine surgery: A technical note. NMC Case Report Journal. 9, 249-253 (2022).
- Zhou, C., et al. Unique complications of percutaneous endoscopic lumbar discectomy and percutaneous endoscopic interlaminar discectomy. Pain Physician. 21 (2), 105-112 (2018).
- Wasinpongwanich, K., et al. Full-endoscopic interlaminar lumbar discectomy: Retrospective review of clinical results and complications in 545 international patients. World Neurosurgery. 132, 922-928 (2019).
- Yin, J., Jiang, Y., Nong, L. Transforaminal approach versus interlaminar approach: A meta-analysis of operative complication of percutaneous endoscopic lumbar discectomy. Médecine. 99 (25), 20709 (2020).
- Manabe, H., et al. Thermal annuloplasty using percutaneous endoscopic discectomy for elite athletes with discogenic low back pain. Neurologia Medico-Chirurgica. 59 (2), 48-53 (2019).
- Wang, L., Li, L., Cheng, C., Xue, Y. The percutaneous spinal endoscopy "isolation zone" technique for discogenic low back pain: a case series study. European Journal of Medical Research. 27 (1), 200 (2022).
- Tonosu, J., et al. Diagnosing discogenic low back pain associated with degenerative disc disease using a medical interview. PLoS One. 11 (11), 0166031 (2016).
- Momenzadeh, S., et al. The effect of percutaneous laser disc decompression on reducing pain and disability in patients with lumbar disc herniation. Journal of Lasers in Medical Sciences. 10 (1), 29-32 (2019).
- Zhang, Y., et al. Comparison of endoscope-assisted and microscope-assisted tubular surgery for lumbar laminectomies and discectomies: Minimum 2-year follow-up results. BioMed Research International. 2019, 5321580 (2019).
- Liu, K. C., et al. Using percutaneous endoscopic outside-in technique to treat selected patients with refractory discogenic low back pain. Pain Physician. 22 (2), 187-198 (2019).
- Zuo, R., et al. The clinical efficacy of biportal endoscopy is comparable to that of uniportal endoscopy via the interlaminar approach for the treatment of L5/S1 lumbar disc herniation. Frontiers in Surgery. 9, 1014033 (2022).
- Yuan, C., Wen, B., Lin, H. Clinical analysis of minimally invasive percutaneous treatment of severe lumbar disc herniation with UBE two-channel endoscopy and foraminal single-channel endoscopy technique. Oxidative Medicine and Cellular Longevity. 2022, 9264852 (2022).
- Minamide, A., et al. Microendoscopic decompression for lumbar spinal stenosis with degenerative spondylolisthesis: The influence of spondylolisthesis stage (disc height and static and dynamic translation) on clinical outcomes. Clinical Spine Surgery. 32 (1), 20-26 (2019).
- Yeung, A. T., Yeung, C. A. In-vivo endoscopic visualization of patho-anatomy in painful degenerative conditions of the lumbar spine. Surgical Technology International. 15, 243-256 (2006).
- Shi, C., et al. Development of an in vivo mouse model of discogenic low back pain. Journal of Cellular Physiology. 233 (10), 6589-6602 (2018).
