A standardized burn device was used to create full-thickness burn wounds at 150 °C for 1 min, which resulted in a homogenous deep burn with a uniform margin of erythema and inflammation (Figure 3 and Figure 7). Each pig received eight full-thickness burn wounds on their back, as depicted in Figure 3C.
The non-invasive real-time assessment of the burn wounds by B-mode high-resolution ultrasound to confirm the wound depth and progression of wound healing over time showed the destruction of all skin layers up to the subcutaneous fat (Figure 4). Laser speckle imaging (LSI) was used for further characterization of the wound perfusion (Figure 4A).
The burn wounds showed a thick pyogenic membrane on the wound surface by day 7 post-inoculation, thus confirming the infection and the establishment of the burn wound biofilm (Figure 7A). Digital planimetry showed an increased wound area at day 3 post-inoculation with PAO1 due to the inflammatory response at the wound site and margins (Figure 7A,B). Although the wound area started to shrink by day 14 post-inoculation, incomplete healing to approximately 25% of the original wound size was observed at day 56, indicating the chronicity of the wounds (Figure 7B). Wound chronicity and impaired wound healing were further confirmed by the TEWL, which showed high transepidermal water loss. The TEWL results reflected the loss of skin barrier function compared to normal skin at all measured the timepoints, thus indicating functional impairment of the burn wound healing (Figure 7B). This was also confirmed by the suppression of the tight junctional proteins ZO-1 and 213 and the impairment of the restoration of skin barrier function, as reflected in the high TEWL values seen at day 35 (mid) and day 56 (late) despite the visual wound closure (Figure 7I).
The burn depth was further validated by H&E staining, which showed distortion and necrosis of all the histological skin layers, as shown in Figure 7C. The established biofilm of PA01 was further validated at day 7 post-inoculation by CFU (Figure 7E,F), SEM imaging (Figure 7G), and immunofluorescence staining (Figure 7H).

Figure 1: Setup for the procedure. (A) Surgical table preparation. (B) Ear vein cannulation for IV fluids and drug administration. (C) Thermal blanket covering to protect the pig from hypothermia during the procedure. (D) Burner and timer setup. Please click here to view a larger version of this figure.
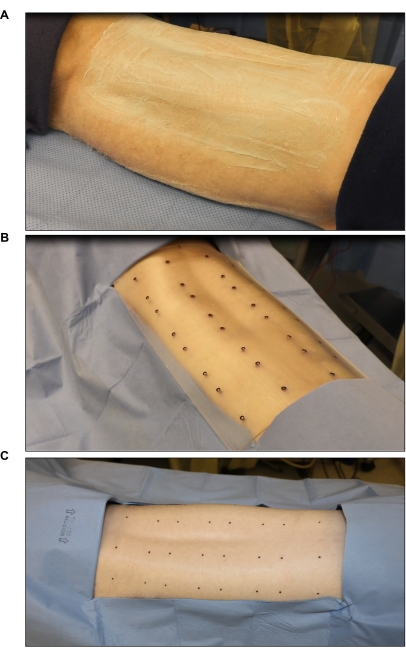
Figure 2: Surgical site sterilization and marking. (A) Hair clipping and sterilization. (B) Marking of the burn site using a sterile eight-wound standard template (each wound is 2 in x 2 in). (C) Final marking using a sterile skin marker. Please click here to view a larger version of this figure.
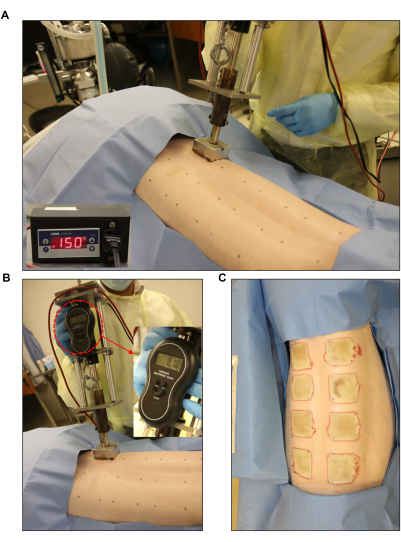
Figure 3: Burn wound induction. (A,B) Standardized burner with a pressure gauge and automated controller unit (2 in x 2 in) applied to the pre-marked wound site. (C) The whole back showing the eight full-thickness burn wounds. Please click here to view a larger version of this figure.
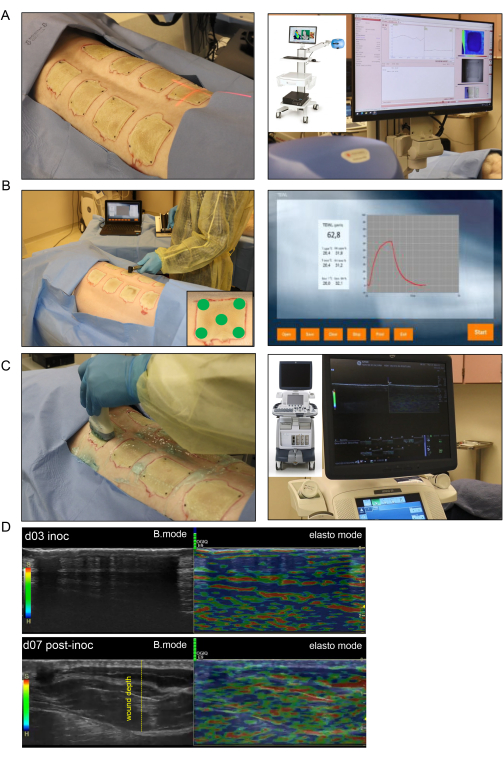
Figure 4: Noninvasive burn wound imaging and assessment. (A) Laser speckle imaging (LSI) with proper orientation of the laser beam indicator to the center of the wound is shown in the left-side image; the right-side image shows the LSI device and the real-time skin vascular perfusion map. (B) Transepidermal water loss (TEWL) probe application to the wound site at five different spots (four wound corners and the center demonstrated in lower-right corner image) is shown in the left-side image; the right-side image is a representative real-time captured screen of the TEWL measurement. (C) Harmonic ultrasound scanning of the burn wound using a high-resolution 16 MHz ultrasound probe is shown on the left side; the right-side image shows the ultrasound device and the real-time screen recording. (D) Structural (B-mode images, grayscale ultrasound) and biomechanical (elastography, color ultrasound) images of the burn wound site at the inoculation day and day 7 post-inoculation. The wound depth is indicated by the yellow dashed line. Please click here to view a larger version of this figure.
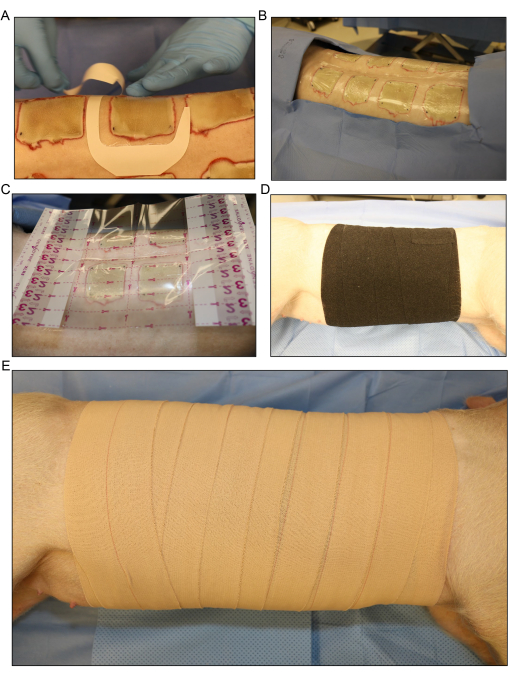
Figure 5: Wound dressing and bandaging. (A) Application of the transparent film dressing for each wound separately. (B) All the dorsal inoculated burn wounds are covered with the first layer of dressing. (C) A larger transparent film dressing is placed over the entire wound area.(D) Application of the second layer of gauze and a loose layer of stretchy elastic bandage around the entire trunk of the pig to absorb any fluid exudate that comes from the wounds. (E) Covering of the entire wound area with a final layer of 4 in adhesive dressing. Please click here to view a larger version of this figure.
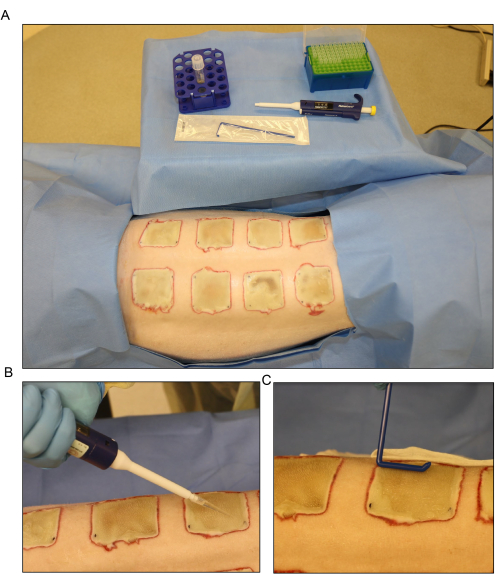
Figure 6: Bacterial inoculation. (A) Setup for the Pseudomonas aeruginosa (PA01) inoculation at day 3 post-burn. (B) Topical application of the inoculum with a pipette using a 500 µL volume for each wound. (C) The inoculum is dispersed across the wound surface evenly using a sterile disposable spreader. Please click here to view a larger version of this figure.
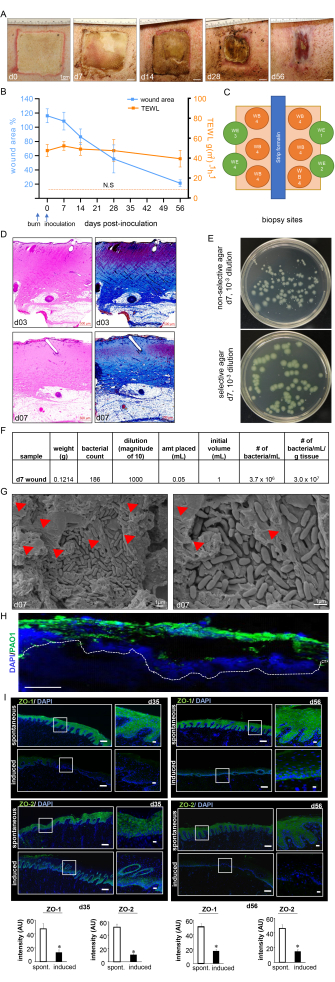
Figure 7: Wound healing progress and biofilm confirmation. (A) Representative images of the wound closure over the timeline of the study. Scale bar = 1 cm. (B) Quantitation of the wound area and TEWL measurements over the timeline of the study (n = 6). The data are represented as mean ± SD. N.S. refers to the TEWL value of normal skin. (C) Schematic diagram showing different wound biopsy sites. D. H&E staining with its corresponding Masson's trichrome staining showing distortion and necrosis of all the skin layers at day 3 post-burn and day 7 post-inoculation. Scale bar = 500 µm. (E) Representative digital images of non-selective agar (Luria-Bertani agar) and selective agar (Pseudomonas Isolation Agar) with bacterial colonies grown from porcine wound bed tissue. The selective medium enables the accurate counting of the PA01 colonies only. (F) A sample colony forming unit (CFU) calculation from the colony counts taken from processed day 7 post-inoculation wound biopsies is shown. (G) Representative scanning electron microscopy (SEM) images of the inoculated burn wounds at day 7 post-inoculation showing the established PA01 biofilm, with a zoomed-in image on the right side. Scale bar = 1 µm. The red arrowheads point to extracellular polymeric substances (EPS). (H) P. aeruginosa on the burn wounds were visualized using anti-Pseudomonas (green) antibody; the immunofluorescence images of the day 7 post-inoculation wound biopsies show heavy colonization of the wound tissues by P. aeruginosa. Scale bar = 100 µm. (I) Representative mosaic (scale bar = 200 µm) and corresponding zoomed-in (scale bar = 50 µm) images of ZO-1- and ZO-2-stained sections on day 35 and day 56 post-inoculation, demonstrating reduced expression of the proteins following the induced infection. The OCT-embedded frozen sections (10 µm) were stained using anti-ZO-1 (green) or anti-ZO-2 (green). The sections were counterstained using DAPI. The bar graphs present the quantitation of the ZO-1 and ZO-2 signal intensity. The data are presented as mean ± SD (n = 3); * p < 0.05 compared to spontaneous ones. Mann-Whitney or Kruskal-Wallis one-way analysis of variance tests were performed to test the significance. Figure 7H,I has been modified from Roy et al.13. Please click here to view a larger version of this figure.
