Detection of H. pylori infection and antibiotic resistance in stomach fluid by qPCR
We performed qPCR for the detection of H. pylori infection by amplifying the ureA gene and determined its antibiotic resistance profile by targeting point mutations in the 23S rRNA gene and gyrA gene (Table 1). The quality control CT values in all three groups of the qPCR experiments were within the recommended range, indicating that the samples were all in a normal state at the time of the experiment and that the test results were reliable. In this study, five samples with different test results (S1-S5) were selected to characterize the reliability of the experimental protocol. S1 represents a representative strain of H. pylori without infection, while the S2-S5 samples are those infected with H. pylori with different resistance results (Figure 1). We set the system not to perform further resistance testing with the samples not infected with H. pylori, so the S1 sample did not enter the resistance test after the system test showed a negative result for H. pylori. In terms of the samples positive for H. pylori infection, the S2 CT values were all within the detection range, indicating that the sample was H. pylori-positive and showed dual resistance to clarithromycin and levofloxacin, and clinicians were recommended to choose other methods for treatment at their discretion. The S3 CT values were within the detection range for H. pylori infection and the levofloxacin resistance test, while no CT values were detected in the clarithromycin resistance test, indicating that the S3 sample was from a levofloxacin-resistant patient. Similarly, the CT value of the S4 sample was within the detection range for H. pylori infection and clarithromycin resistance, while no CT value was detected for levofloxacin resistance, indicating that this patient was resistant to clarithromycin, and it was recommended that they take levofloxacin for treatment. Finally, the S5 sample test showed CT values within the detection range only for the detection of H. pylori infection, indicating that this patient was sensitive to both antibiotics and could be treated using either of the two drugs. Compared to the bacterial culture method, which also detects H. pylori infection and drug resistance, this method is safe and effective in detecting H. pylori infection and drug resistance without causing damage to the patient and can be used to guide the doctor in formulating an appropriate treatment plan.
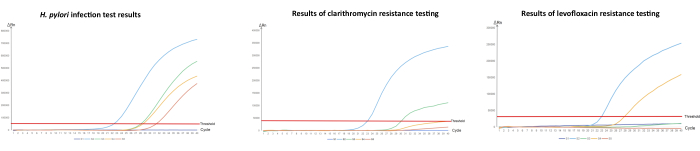
Figure 1: Detection of H. pylori and its antibiotic resistance in stomach fluid by qPCR.
(A) Quantitative PCR amplification of H. pylori infection, (B) detection of clarithromycin resistance, and (C) detection of levofloxacin resistance. "S" stands for sample. "S1" is a sample that came back negative for H. pylori infection and was also tested for antibiotic resistance; "S2" is an H. pylori-infected sample with resistance to both clarithromycin and levofloxacin; "S3" is also an H. pylori-positive sample but is clarithromycin-susceptible and levofloxacin-resistant; "S4" is also an H. pylori-positive sample but is clarithromycin-resistant and levofloxacin-susceptible; "S5" is an H. pylori-positive sample but is susceptible to both clarithromycin and levofloxacin. The concentration of the weak quality control is 1.0 x 103 copies/mL, while the concentration of the strong quality control is 1.0 x 108 copies/mL. Please click here to view a larger version of this figure.
| Sample | H. pylori | Clarithromycin | Levofloxacin | |||
| +/- | CT | +/- | CT | +/- | CT | |
| S1 | – | U | – | U | – | U |
| S2 | + | 22.61 | + | 22.77 | + | 23 |
| S3 | + | 28.32 | – | U | + | 30.18 |
| S4 | + | 28.76 | + | 27.67 | – | U |
| S5 | + | 31.59 | – | U | – | U |
Table 1: Table showing the qPCR results of the detection of H. pylori infection and resistance to clarithromycin and levofloxacin. This table presents the qualitative results for H. pylori infection, the detection of 23S rRNA gene mutations showing that the isolate is resistant to clarithromycin, and the detection of gyrA gene mutations showing that the isolate is resistant to levofloxacin. +/−, qualitative result; +, positive result; −, negative result.
