Based on our experience, proficiency in this model typically requires approximately 2 months of training. Once proficiency is achieved, the donor procedures typically require 15 min, while the recipient procedures require approximately 30 min. The expected mortality rate for a trained operator is 0%.
In Figure 4A, a tracheal allograft exhibits complete obstruction with fibroblastic tissue, and the epithelial cells are visibly destroyed. Conversely, in Figure 4B, a tracheal isograft remains patent, and the epithelial cells are preserved.
Figure 5 illustrates a lung in which the tracheal allograft has been transplanted, showing the presence of lymphoid aggregates.
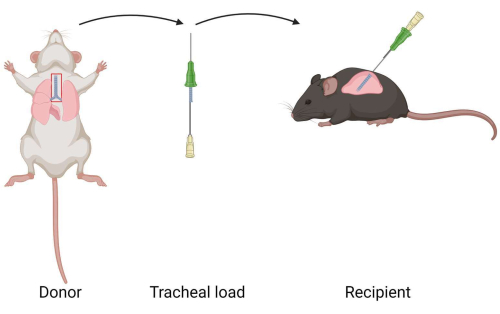
Figure 1: Diagram of murine intrapulmonary tracheal transplantation model. A tracheal allograft is extracted from a donor mouse. The tracheal allograft is loaded into a catheter. The tracheal allograft is transplanted to the lung of a recipient. Please click here to view a larger version of this figure.

Figure 2: Position of the recipient during surgery. The mouse is placed in a right lateral decubitus position. The recipient mouse's head is oriented away from the surgeon and the tail faces the surgeon. Please click here to view a larger version of this figure.
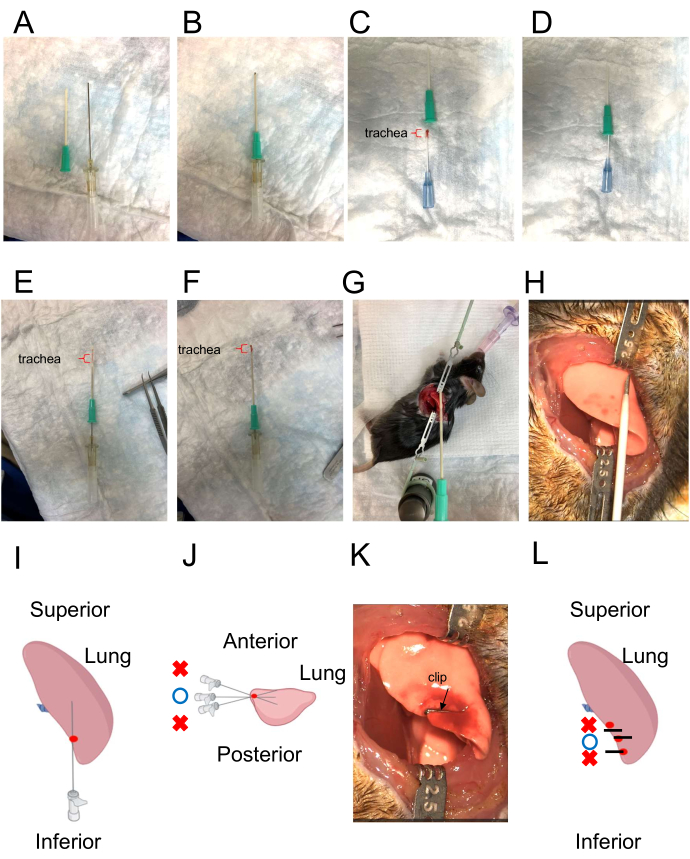
Figure 3: Catheter for tracheal insertion and illustration of the direction of the insertion of the tracheal graft. (A) The catheter for tracheal insertion. The outer catheter has a sharp tip (left), while the inner catheter has a blunt tip (right). (B) Combination of outer and inner catheters. The inner catheter protrudes slightly from the outer catheter. (C,D) Loading the donor trachea into the catheter. The red bracket indicates the tracheal graft. (E) Tracheal graft inside the catheter. The red bracket indicates the tracheal graft. (F) Extruding the inner tracheal graft using the inner catheter as a "pusher." The red bracket indicates the tracheal graft. (G, H) Simulation of the direction for placement of the tracheal graft. (I,J) Creating the pathway using a 22 G needle. The depth should closely match the length of a tracheal allograft. The needle's direction should be opposite from the surgeon and parallel to the tabletop. The correct puncture site is denoted by the red point. The appropriate insertion angle is indicated by the blue circle. Incorrect angles are indicated by red crosses. (K,L) Closing the pleural injection site with a clip. Black lines represent clips. Red point represents the puncture site. The blue circle indicates the correct clipping point. Red crosses indicate incorrect clipping points. Please click here to view a larger version of this figure.
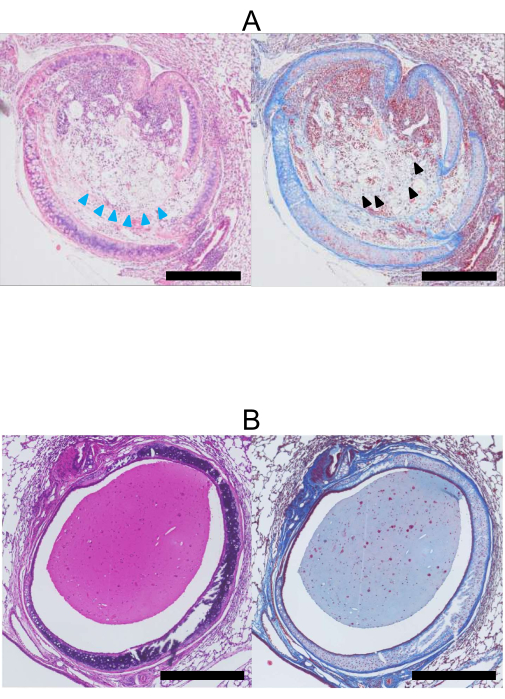
Figure 4: Histopathology at 28 days post lung transplantation. (A) H&E (left) and Masson's Trichrome (right) stained images of a tracheal allograft (Donor: BALB/c, Recipient: C57BL/6). The lumen of the allograft is occluded with collagen and fibrous tissue stained blue by Masson's Trichrome (black arrowhead). Additionally, the epithelial cells have been lost (blue arrowheads). (B) H&E (left) and Masson's Trichrome (right) stained images of a tracheal isograft. In contrast to the allograft, the lumen of the isograft (Donor, Recipient: C57BL/6) remains open, and the epithelial cells are preserved. Stained tissue is mucus. Scale bars = 500 µm. Abbreviation: H&E = hematoxylin and eosin. Please click here to view a larger version of this figure.
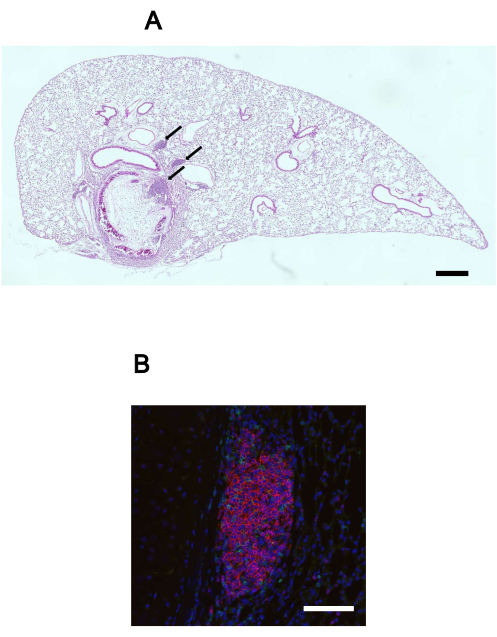
Figure 5: Lymphoid aggregates in the lung with the transplanted tracheal allograft. (A) H&E stained image of a lung with a transplanted tracheal allograft in situ. Lymphoid aggregates (black arrows) are observed within the lung tissue. Scale bar = 500 µm. (B) Immunofluorescence image of a lymphoid aggregate, highlighting the presence of B cell (B220, red), T cell (CD3, green), and nuclei (DAPI, blue). Scale bar = 100 µm. Abbreviations: H&E = hematoxylin and eosin; DAPI = 4',6-diamidino-2-phenylindole. Please click here to view a larger version of this figure.
