The subsequent representative results are derived from biopsies taken from the benign epithelium of both the gastric body and gastric antrum regions of the stomachs of five different patients undergoing upper endoscopy. Two to four "domes"/wells were plated and analyzed per patient for both gastric body and antrum biopsies. Organoids were successfully generated from the gastric body and gastric antrum biopsy tissue from all five patients. On average, 41 organoids were analyzed per "dome"/well. All images are z-projections acquired using a confocal microscope, and the quantification of organoid size and sphericity was performed using commercially available image analysis software (see Table of Materials).
Organoids are generally identifiable within 10 days post-seeding of single cells (Figure 3A). By day 20, the organoids are large and typically need to be passaged. While the number of organoids that form post single-cell seeding can be somewhat variable, expected results for the number of organoids formed from body and antral gastric biopsies are shown in Figure 3B. The number of body and antral organoids peaks at day 10 post-seeding. While not significant, the total number of organoids begins to decrease from day 10 to day 15 and day 15 to day 20. There appears to be a subpopulation of small organoids that form by day 10 and then cease growth and die off over the following 10 days, which would explain this trend. Importantly, it is shown that the number of organoids formed from antral biopsy tissue is significantly higher than biopsy tissue from the body at days 10, 15, and 20. The number of antral organoids formed was on average 2-fold higher than the number of organoids formed from the body.
In Figure 3C, representative results for organoid growth after single-cell seeding between day 10 and day 20 are shown. While organoids from both antral and body biopsies saw steady growth from day 10 to 20, organoids generated from antral biopsy tissue displayed a greater growth rate compared to organoids generated from body biopsy tissue. In particular, antral organoids had nearly a 4-fold greater area than body organoids at day 20.
Across different patients, a diversity of organoid morphology is typically observed in any single "dome"/well (Figure 4A). Some organoids are more round or spherical while others displayed a more irregular morphology. However, on average, sphericity, a measurement of how spherical an organoid is (where a score of 1 = a perfect sphere)18, showed little variation within and between organoids generated from body or antral biopsy tissue (Figure 4B). Therefore, although there are differing growth rates, there are typically no significant morphological differences between organoids generated from biopsy tissue of the gastric body or antrum.
By day 20 post-initiation, gastric organoids are typically ready to be passaged. A large organoid size (≥1500 µm in diameter) or a darkened interior (suggestive of extensive cellular turnover) of the organoid are key signs that organoids need to be passaged (Figure 5A). Organoids left to go beyond this point may begin to break down into 2D monolayers (Figure 5B) that do not reliably re-form organoids after passaging, perhaps indicating a loss of viability or stemness. After passaging and reseeding gastric organoids using the fragmentation protocol described herein, the "domes" will contain many organoid fragments (Figure 5C) that will reorganize themselves into many more organoids and grow much more quickly compared to the initial seeding of single cells (Figure 5D). If organoid growth still needs characterization and/or standardization at the time of passaging, gastric organoids can instead be digested to single cells, as previously described19.
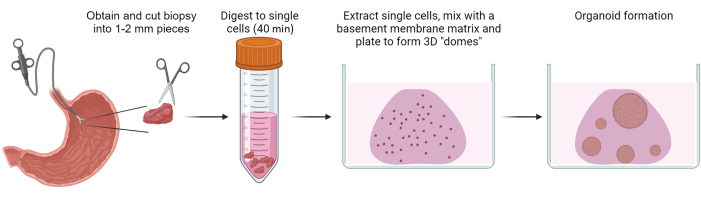
Figure 1: Generation of gastric patient-derived organoids. Schematic overview depicting the process of generating gastric patient-derived organoids from biopsies of benign gastric epithelium. Please click here to view a larger version of this figure.
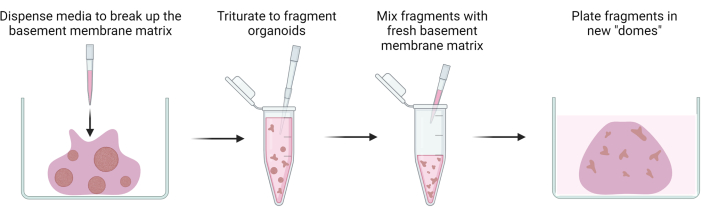
Figure 2: Passaging of gastric patient-derived organoids. Schematic overview illustrating the passaging of gastric patient-derived organoids through fragmentation. Please click here to view a larger version of this figure.
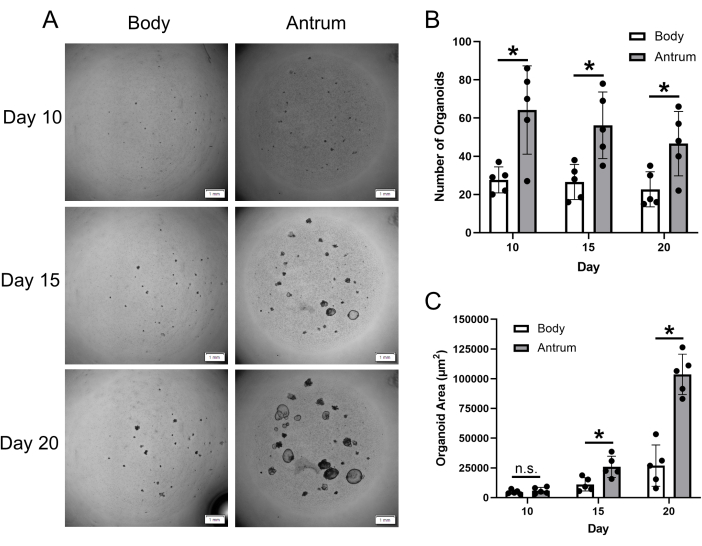
Figure 3: Gastric patient-derived organoid formation and growth. (A) Representative z-projection images displaying the growth of gastric organoids at day 10, 15, and 20 post-single-cell seeding. Images are of organoids generated from gastric body and antrum biopsy tissue from the same patient. Scale bar = 1 mm. (B) Mean (±SD) number of gastric body and antrum organoids at indicated timepoints post-single-cell seeding. (C) Mean (±SD) area (µm2) of gastric body and antrum organoids at indicated timepoints post-single-cell seeding. n = 5 patients per group and timepoint. * = statistically significant difference (p ≤ 0.05) at the indicated timepoint. n.s. = no statistically significant difference at the indicated timepoint. Statistical comparisons conducted via 2-way ANOVA. Please click here to view a larger version of this figure.
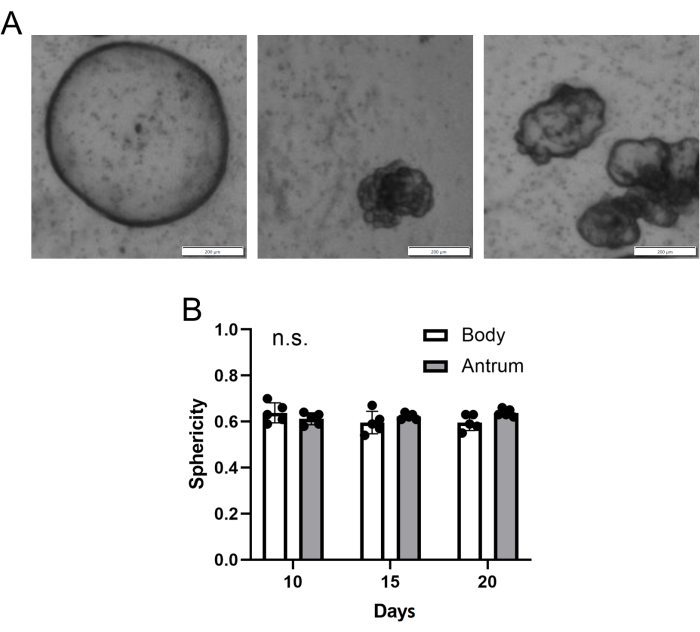
Figure 4: Gastric patient-derived organoid morphology. (A) Representative z-projection images of different gastric organoid morphologies from an individual "dome"/well of gastric body-derived organoids at day 15 post-single-cell seeding. Scale bar = 200 µm. (B) Mean (±SD) gastric body and antrum organoid sphericity (where a value of 1 = a perfect sphere). n = 5 patients per group and timepoint. n.s. = no statistically significant difference at any timepoint. Statistical comparisons conducted via 2-way ANOVA. Please click here to view a larger version of this figure.
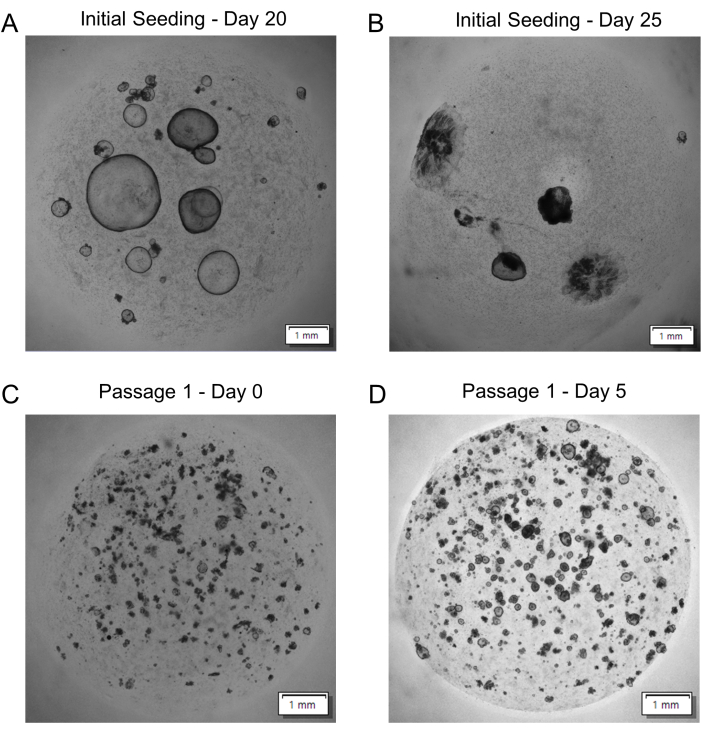
Figure 5: Gastric patient-derived organoid passaging. (A) Representative image of organoids ready to be passaged at day 20 post-single-cell seeding. (B) Representative image of organoids overdue for passaging at day 25 post-single-cell seeding. (C) Representative image of fragmented organoids after reseeding (Passage 1 – Day 0). (D) Representative image of organoid growth over 5 days after reseeding (Passage 1 – Day 5). All images are z-projections. Scale bars = 1 mm. Please click here to view a larger version of this figure.
Supplementary Table 1: Solutions and media recipes. Please click here to download this File.
