Surgical Methods
1. Surgical Preparation and Anesthesia
- Set up the sterile surgical field with the necessary surgical instruments: shaving shears, forceps with teeth, fine atraumatic forceps, fine needle driver, gauze, Metzenbaum scissors, tenotomy scissors, scalpel blade, 30 gauge hypodermic needle, saline filled 1 mL syringe, four 6-0 polypropylene sutures, 7-0 polyglactin suture, 4-0 polyglactin suture.
- Anesthetize the animal with isoflurane inhalation in the induction chamber. Confirm complete induction of the animal before transferring to the surgical field. Ensure that the inhalational anesthesia tube is in appropriate position to have continuous anesthesia.
- Place the animal supine on the sterile drape.
[For cystometric analysis, see section below in tunneling the cystostomy catheter.] - Use the shaving shears to remove the fur from the lower abdomen.
- Prep the abdomen with betadine and 70% ethanol.
- Prior to incision, an analgesic such as buprenorphine (0.05-0.1 mg/kg) can be injected subcutaneously for perioperative pain control.
2. Incision and Exposure of the Bladder
- Make a 1-2 cm (dependant on size of animal and whether rat or mouse) lower midline incision with the scalpel through the skin. Deepen the incision at the lower portion of the incision through the rectus muscle taking care not to injure the underlying bowel or bladder.
- Using toothed forceps, elevate the rectus muscle and dissect free the posterior surface of the muscle with fine Metzenbaum scissors.
- Incise the remainder of the muscle in the midline for the entire length of your skin incision.
- Deliver the bladder through the incisional wound (Figure 1). The bladder is usually the most dependent organ in the pelvis. (In the male, the prostate is actually more dependent and is larger than the decompressed bladder.)
- Place one stay suture through the posterior wall of the bladder, and then another through the anterior wall of the bladder using 6-0 polypropylene suture. Place additional sutures laterally. Do not tie these sutures. When the sutures are held taut, the bladder will have a square configuration measuring approximately 1 cm2 (Figure 2). Be careful not to have too much tension on these sutures as they can easily be pulled through the bladder tissue.
- Incise the bladder longitudinally through the anterior bladder wall (just inferior to the dome of the bladder) in the midline for approximately 1 cm (1.5-2 cm in the rat bladder).
3. Anastomosis of the Scaffold
- Using fine scissors, trim the silk scaffold to the approximate area of the bladder defect.
- Using 7-0 polyglactin suture, start at one corner of the scaffold and suture it to the bladder in a continuous, running fashion to create a watertight seal all the way around the defect (Figure 3).
- Test the integrity of the anastomosis by filling the bladder with sterile saline by instilling it through the wall of the bladder with a 30 gauge hypodermic needle. If a leak is found, this can be closed with an additional interrupted 7-0 polyglactin suture to close the gap.
- Reduce the reconstructed bladder back into the abdomen.
4. Incisional Closure
- Prior to closure of the abdominal wall, inject the rectus muscle and subcutaneous tissue with bupivicaine for local anesthesia (< 3 mg/kg of 0.25%).
- Reapproximate the rectus muscle with a continuous, running 4-0 polyglactin suture.
- Close the skin with a continuous, running 4-0 polyglactin suture.
- Clean and dry the incision (Figure 4).
- Transfer the animal into a warm, clean cage for awakening from the anesthesia.
The steps for cystostomy catheter placement for cystometric analysis are as follows:
5. Tunneling the Cystostomy Catheter
- Set up the sterile surgical field with the necessary surgical instruments: shaving shears, forceps with teeth, fine atraumatic forceps, fine needle driver, gauze, Metzenbaum scissors, tenotomy scissors, small curved clamp, scalpel blade, 6-0 polypropylene, 4-0 polyglactin suture, 3-0 silk suture (4-0 silk suture for mice), 18G needle, 22G blunt tip needle, 25G needle, 1 mL saline filled syringe, polyethylene tubing 50 (PE-50) cut for a length of ~10 cm.
- Flare the end of the PE-50 tubing by gently exposing it to a flame. Be careful not to melt the end off or occlude the lumen (this can be verified by injecting saline through a 25G needle connected to the “non-flared” end and ensuring flow). This serves as an anchor to maintain the tube within the bladder (Figure 5).
- Anesthetize the animal as above in step 1.2.
- Use the shaving shears to remove the fur from both the dorsum of the animal between the scapula and the lower abdomen on the ventrum.
- Prep the areas with betadine and 70% ethanol. Place the animal prone on the drape.
- Make a 1 cm incision on the dorsum between the scapula. Using the Metzenbaum scissors, develop a plane between the skin and the underlying muscle by placing the tips of the scissors in the plane and spreading them to create a tunnel around to the ventral abdomen.
- Reposition the animal supine. Make your abdominal incision and expose the bladder as above in steps 2.1-2.4. Reduce the bladder back into the abdomen.
- Place a small clamp into your subcutaneous tunnel created in step 5.6 starting from your dorsal skin incision. Using your fingers to protect the intra-abdominal contents, pierce through the abdominal wall with the tips of the clamp into the abdomen.
- Grasp the smooth end of the PE-50 tubing with the clamp and pull it back through the dorsal incision. Ensure that the bulbed end is not pulled past the abdominal wall (Figure 6).
6. Placing the Cystostomy Tube
- Deliver the bladder through the incision. From this point on, the bladder should be handled with fine forceps to prevent trauma to the bladder that could cause damage or inflammation that can skew your cystometric results or result in additional discomfort for the animal post-operatively.
- Make note of the proposed site for the cystostomy tube. It should be placed at the dome of the bladder (superior to the augment segment). This will prevent kinking or occlusion of the tube.
- Using the 6-0 polypropylene suture, place a pursestring stitch at the dome of the bladder in the following manner: place the first throw through the wall of the bladder longitudinally, lateral to the proposed site for the cystostomy tube. Leave a small clamp on the loose end so that the suture is not inadvertently pulled all the way through. Place the next throw in a transverse direction, starting first going into the bladder wall slightly lateral to the exit of your first throw.
- Do not pull the suture taut. Place your next suture parallel to your first (longitudinally) going into the bladder just cephalad to the exit site of your last, transverse suture. The fourth throw will start lateral to the exit of the last stitch and end next to the entrance for your very first throw. Done correctly, this forms a circumferential square around the proposed catheter site (Figure 7).
- Using an 18G needle, pierce the bladder wall in the center of the pursestring suture. Be careful not to pierce too deeply (just enough to be intraluminal). Place the tips of your fine forceps in the opening and gently spread to widen the hole.
- Insert the bulbed end of the catheter into the defect in the bladder until it is intraluminal. Pull the pursestring suture tight around the catheter and tie it down. This should cinch the bladder wall around the catheter keeping it in place (Figure 8).
- Take one end of the suture and wrap it around the catheter once and tie this down to further secure the catheter.
7. Testing the Catheter and Closing the Abdominal Incision
- With a 1 mL syringe and 25G needle, insert the needle into the tubing and slowly inject saline to distend the bladder. Observe for leaking around the catheter. Once you see leaking from the urethra, aspirate the saline to decompress the bladder again.
- Close the abdominal incision as above in steps 4.1-4.4.
8. Closing the Dorsal Incision and Securing the Catheter (For rats)
- Reposition the animal prone.
- Cut the catheter tubing at the level of the skin with the scissors. Insert a 22G blunt tip needle into the tubing.
- Close the skin over the tubing with 4-0 polyglactin in a running fashion. Leave the needle hub extruding from the skin.
- Place an intravenous line cap on the blunt needle. Using 3-0 silk suture, secure the catheter tip to the skin (Figure 9).
- Clean the incision. Transfer the rat into a warm, clean cage for awakening from the anesthesia.
8.* Closing the Dorsal Incision and Securing the Catheter (For mice or rats)
- *Occlude the distal end of the catheter by kinking it or using a flame to melt the end.
- *Coil the end of the tubing and leave it in the subcutaneous pouch on the dorsum of the animal (do NOT cut tubing to shorten it) (Figure 10).
- *Close the skin over the tubing with 4-0 polyglactin in a running fashion (Figure 11).
- *On the day of cystometry, prepare the dorsal incision with betadine and 70% ethanol. Open the dorsal incision under anesthesia and remove the coiled tubing from the subcutaneous pouch. Close the incision. Awaken the animal from anesthesia and perform cystometry when it is fully awake.
9. Representative Results – Surgical Methods
The reconstructed bladder should be as water-tight as possible to avoid complications related to a significant urinary leak (Figure 3). Pain or discomfort usually manifest as shivering or scratching and gnawing at the abdominal incision. This can be managed with daily subcutaneous injections of a non-steroidal anti-inflammatory such as meloxicam (0.5-1.0 mg/kg subcutaneous). Typically, the animals only require the injections for the first 3 days post-operatively. This can be supplemented with an opioid, such as buprenorphine (0.05-0.1 mg/kg subcutaneous every 8-12 hr) as needed. The animals should be monitored 3 times daily for the first 3 post-operatively days, twice daily for post-operative days 3-5 and then daily thereafter to evaluate for pain, signs of infection, adequate wound healing, activity, grooming, and skin turgor. Antibiotics (Baytril, 5mg/kg subcutaneous every 24 hr in a volume not exceeding 0.1 mL) are given for the first 72 hr following surgery, as surgical prophylaxis against infection. Signs of normal recovery are normal ambulation and activity levels, appropriate feeding and drinking, absence of pain or distress (no vocalization) and normal socialization with cagemates. A recovery time of at least 5-7 days should be given before cystometric analysis, to allow for bladder healing and decreased inflammation which could potentially affect the results.
Cystometric Analyses
10. Awake Cystometric Analysis
- Setup described with MLT844 ADInstruments with data capture and analysis with LabChart v6 (ADInstruments) and infusion with a Harvard 22 syringe pump (Harvard Apparatus, Holliston, MA), although other comparable systems are available (Figure 12).
- Calibrate both volume and pressure based on the specifications of the cystometric system used.
- Place the animals in metabolic cages (cages with a wire mesh floor) which are suspended over a scale. The scale is connected to a transducer.
- Purge the system of any air bubbles and ensure continuous flow from the infusion pump.
- Connect the data capture system to a computer and observe for data tracings. Adjust the scale accordingly. Bladder pressure and urine volume will be continuously recorded.
- Access the suprapubic catheters with a 27G needle connected via a T-tube to the pressure transducer and the infusion pump. Begin the infusion of physiologic saline at 12.5 μL/min for the mouse and 100 μL/min for the rat.
- Allow the voiding pattern tracing to stabilize (bladder pressure rise, followed by a void). This usually takes approximately 10-20 minutes. Record the micturition cycles for 45-120 minutes or at least 3-4 voiding cycles.
- Observe entire procedure in real-time to troubleshoot for complications that will lead to artifact (i.e. catheter kinking, obstruction, etc; see below discussion).
- Stop the infusion, disconnect the catheter from the system, and return the animal to its cage.
11. Unconscious Cystometric Analysis (No suprapubic catheter)
- Anesthetize the animal with urethane (1-2 g/kg) intraperitoneal injection (IP).
- Expose the bladder as above in steps 1.3-2.4.
- Calibrate the system as in step 9.2. Prepare the system as in step 9.4-9.5.
- Insert a 27G needle connected via a T-tube to the pressure transducer and infusion pump into the lateral aspect of the bladder.
- Record the micturition cycles for 45-90 minutes.
- Stop the infusion, remove the needle from the bladder and euthanize the animal.
12. Representative Results – Cystometric Analyses
Urodynamic tracings can then be analyzed to derive parameters such as voided volumes, compliance, peak voiding pressures, inter contraction interval, micturition cycle time and post void residual volumes.
Cystometrogram can be divided into a filling and a voiding phase. A normal filling phase is the portion of the micturition cycle in which bladder fills with very little change in intravesical pressure. A normal voiding phase of the tracing consists of a steady rise in the intravesical pressure corresponding to the detrusor contraction. The highest pressure reached during the voiding phase of the tracing is termed the peak voiding pressure. A high peak voiding pressure could suggest an obstructive voiding pattern, a hypercontractile bladder or a kink in the SP catheter. Compliance can be calculated by acquiring the ratio of the volume instilled during the filling phase and the change in pressure (compliance = ΔV/ΔP). A hypocompliant bladder is one that is unable to accommodate adequate urinary volumes at low pressures. The intercontraction interval can be calculated by analyzing the time between two contractions as seen on the cystometrogram. A short intercontraction interval is suggestive of an irritable bladder. The micturition cycle time refers to the time it takes for an entire filling and voiding phase to complete and can be easily ascertained by analyzing the tracing. At the conclusion of the cystometry, post-void residual (PVR) can be obtained. This is done by aspirating the suprapubic catheter upon the completion of a detrusor contraction. These parameters help the investigator objectively study the bladder dynamics as the bladder fills and empties.

Figure 1. Photograph of the abdominal incision and extrusion of the bladder.
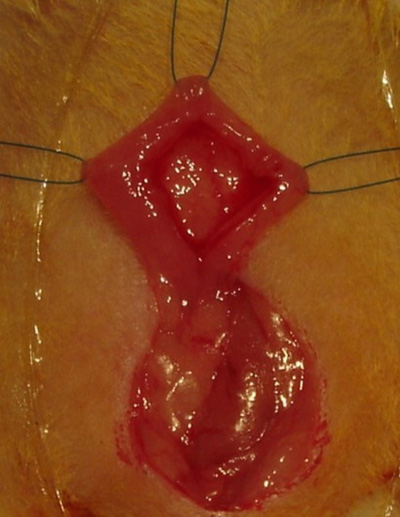
Figure 2. Bladder incision with exposure of the bladder lumen.
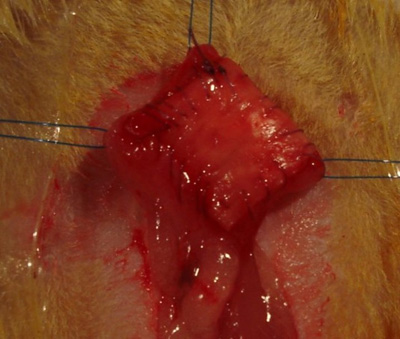
Figure 3. Integration of the implant onto the bladder wall.

Figure 4. Photograph of the closed incision.

Figure 5. Flared end of the PE-50 tubing.
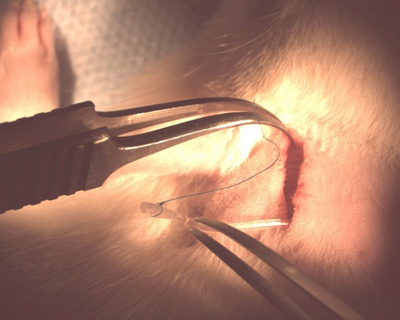
Figure 6. PE-50 tubing (catheter) through the dorsal incision.
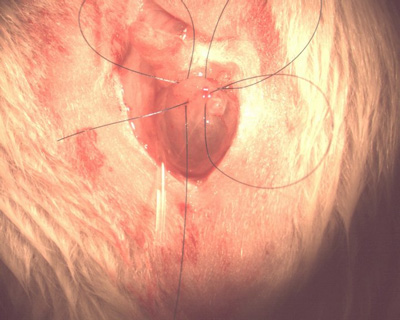
Figure 7. Pursestring suture.
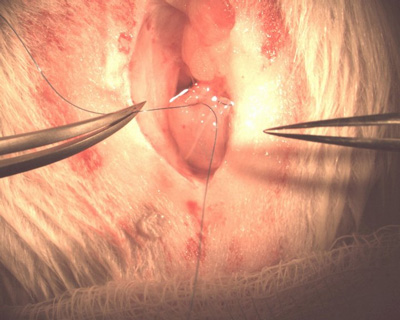
Figure 8. Securing the catheter to the bladder.

Figure 9. Secured catheter hub.

Figure 10. Coiled tubing in subcutaneous pouch.
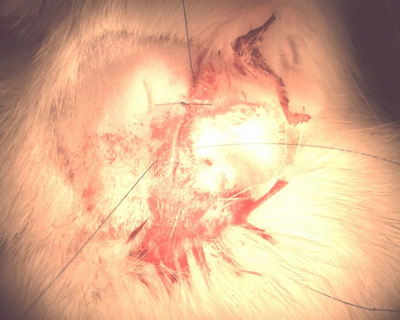
Figure 11. Dorsal incisional closure.

Figure 12. Example cystometric set-up.
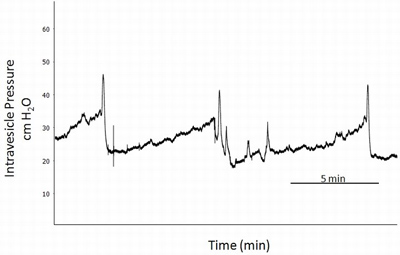
Figure 13. Representative cystometry tracing.
