The reported representative results follow the main in vitro/in vivo assays depicted in the workflow in Figure 1. 48 hr after 4OH-tamoxifen administration MyoD-positive nuclei are identifiable within MyoD-ER transduced IDEMs in culture (Figure 2A). The cells then fuse and differentiate into multinucleated myotubes (Figure 2B). When transplanted intramuscularly into a murine model of acute muscle injury, IDEMs contribute to tissue regeneration (Figure 3). The efficacy of IDEMs in a gene- and cell-therapy setting for murine models of muscular dystrophy was assessed by the treadmill exercise tolerance test: Figure 4 shows the results obtained after transplantation of wild-type MIDEMs into Sgca-null/scid/beige mice, displaying an amelioration of the motor capacity in treated mice7. Ex vivo analyses of transplanted muscles show GFP-positive areas representing the extent of colonization of IDEMs into the host tissue (Figures 5A-C), thus demonstrating that donor cells engraft into dystrophic muscle. Importantly, transplanted cells are able to differentiate in vivo, forming new skeletal myofibers. Indeed Figure 5 shows Sgca expression from genetically corrected HIDEMs into Sgca-null/scid/beige mice (Figures 5D and 5E). Structural amelioration in the architecture of transplanted muscles can be assessed through Masson's trichrome staining: Figure 5F shows a decrease in the amount of fibrotic tissue in treated muscle.
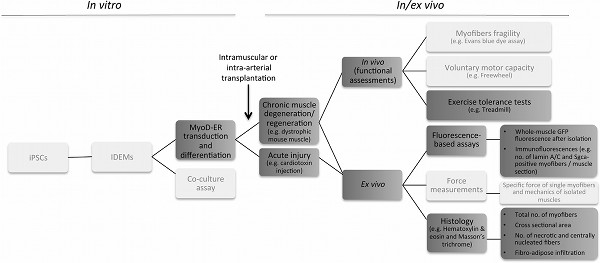
Figure 1. Protocol flow chart. The scheme provides an overview of the IDEM-based strategy, from preliminary in vitro differentiation assays (left) to the various steps necessary to assess engraftment, myogenic potential and functional amelioration in vivo and ex vivo (right). Dark grey boxes contain the various steps described in the protocol; light grey boxes contain parts of the method not detailed in this article. Click here to view larger figure.
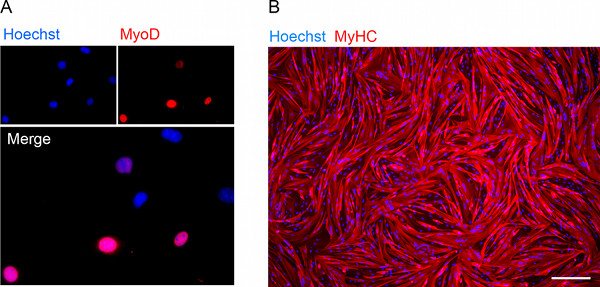
Figure 2. Assessment of myogenic potential in vitro. (A) Immunofluorescence showing nuclear MyoD expression in 4 out of 7 MyoD-ER transduced MIDEM nuclei after 48 hr of exposure to 4OH-tamoxifen. (B) Immunofluorescence staining for myosin heavy chain (MyHC) on 4OH-tamoxifen-induced HIDEM-derived myotubes after one week in differentiation medium (Scale bar, 200 μm). Click here to view larger figure.
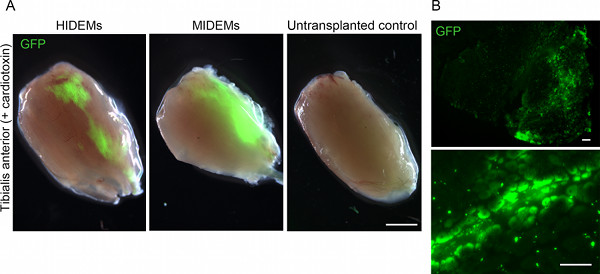
Figure 3. In vivo assessment of cell engraftment in a model of acute muscle regeneration. (A) Stereomicroscopic GFP fluorescence images of freshly isolated cardiotoxin-injured tibialis anterior muscles explanted 2 weeks after intramuscular injection of 106 GFP-HIDEMs (left) and GFP-MIDEMs (center). Scale bar, 2 mm. (B) Low (top) and high (bottom) magnification pictures of the muscle transplanted with MIDEMs shown in (A) displaying GFP-positive myofibers. Scale bar, 200 μm. Click here to view larger figure.
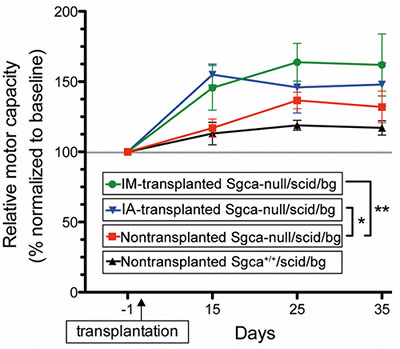
Figure 4. Treadmill exercise tolerance test. Representative treadmill test for transplanted (IM = intramuscular; IA = intra-arterial). Sgca-null/scid/ beige mice (106 cell/injection) versus nontransplanted dystrophic and nondystrophic control immunodeficient mice. The plot shows functional amelioration of dystrophic mice transplanted with MIDEMs (12-22% more than nontransplanted animals 35 days after transplantation). Data are shown as average motor capacity relative to baseline performances (i.e. 100% represents the baseline performance of each group and only treated mice significantly improve it upon repeated measurements). *P < 0.05; **P < 0.005, one-way ANOVA. From previously published work of the authors7. Click here to view larger figure.
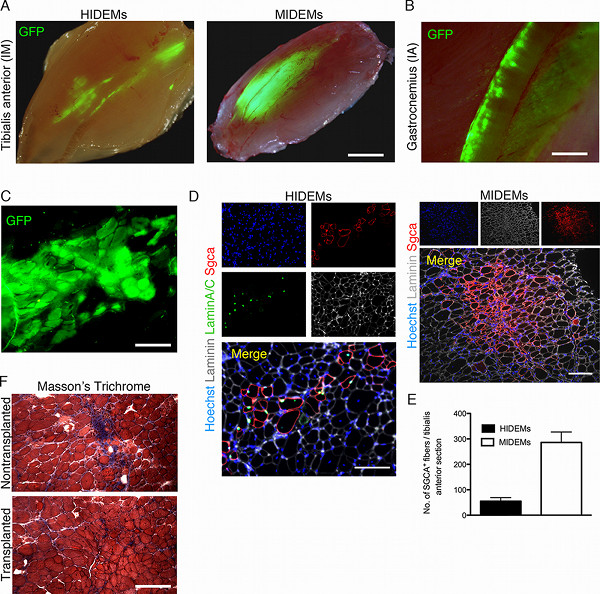
Figure 5. In vivo assessment of engraftment and myogenic potential in mouse models of muscular dystrophy. (A) Stereomicroscopic GFP fluorescence images of freshly isolated tibialis anterior muscles of Sgca-null/scid/beige mice explanted 3-4 weeks after intramuscular injection of 106 human (HIDEMs, left; transplantation in juvenile mice) and murine (MIDEMs; right) GFP-IDEMs. Scale bar, 2 mm. (B) Stereomicroscopic GFP fluorescence image of a freshly isolated gastrocnemius muscle explanted 3 weeks after intra-arterial injection of 106 GFP-MIDEMs. Scale bar, 1 mm. (C) Fresh frozen transverse section of the muscle transplanted with MIDEMs shown in (A) displaying a cluster of GFP-positive myofibers. Scale bar, 200 μm. (D) Immunofluorescence staining on sections of intra-muscularly transplanted muscles (as in A) showing clusters of genetically-corrected fibers, originated from grafted IDEMs. Scale bar, 150 μm. (E) Quantification of α-sarcoglycan (Sgca)-positive myofibers one month after intramuscular transplantation of genetically-corrected IDEMs into Sgca-null/scid/beige mice. (F) Masson trichrome staining of tibialis anterior muscles from transplanted and control Sgca-null/scid/beige mice (red: muscle fibers; blue: fibrosis) highlighting the reduction of the fibrotic infiltrate in treated muscle. Scale bar, 200 μm. Click here to view larger figure.
