During the surgical procedure, ligation of the left coronary artery can be identified by a marked blanching downstream of the occluded artery. As a test before tying the knot, the suture can be tightened briefly to check if it is in the appropriate place. Additionally, since occlusion of the artery results in almost instantaneous decrease in the ability of the left atrium to properly beat, the left atrium will enlarge in response to a backflow of blood in the system.
M-mode echocardiography measurements taken as early as 2 days post-infarction show a cessation of left wall movement, indicative of the muscle reconstruction. Qualitative calculations made from the data show a decrease in ejection fraction and stroke volume in the infarcted hearts. At the termination of the experiment, when the hearts are collected for histological purposes, a clear dilation of the left ventricle can be seen, along with a thinning of the left ventricular wall, and the deposition of collagen that denotes scar tissue deposition in place of functioning cardiomyocytes (Figure 1).
Also seen upon histological analysis is the presence of the hydrogel construct thanks to the administration of the fibrin gel (Figure 2). For our purposes, the adhesive system must be viscous enough to allow precise placement control and minimize subsequent runoff into surrounding organs, but malleable enough not to interfere with heart function. Preliminary tests were performed to calculate the viscosity, gelation time, and stiffness of various fibrinogen/thrombin ratios, in order to determine the proper combination that suits our needs. In vivo analysis was performed to test the ability of the fibrin glue to maintain patch-to-tissue adhesion while still allowing for full heart function (data not shown). It should be noted that the fibrin glue did not harm the myocardium, as evidenced by the lack of tissue remodeling or ventricular thinning at the site (Figure 2). The cardiomyocytes remain intact despite the addition of both a cardiac patch and its accompanying glue. Additionally, viability testing confirmed that that the administration of fibrin glue to the external surface of a cell-encapsulating hydrogel patch did not affect cell survival within the patch (Figure 3).
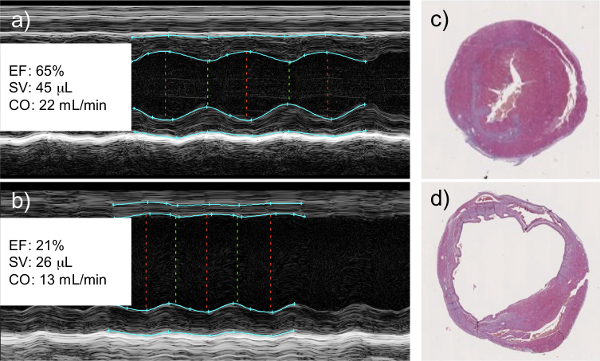
Figure 1: Left Coronary Artery Ligation Results in a Decrease in Cardiac Function as Measured by Echocardiography. M-mode echocardiography of healthy (a) and infarcted (b) hearts. Infarcted hearts show a clear lack of wall movement where viable tissue has been replaced with scar tissue. This correlates with a measureable decrease in left ventricular ejection fraction (EF), cardiac stroke volume (SV), and cardiac output (CO). Histological analysis of healthy (c) and infarcted (d) hearts shows dilation of the left ventricle and thinning of the left ventricular wall of the infarcted myocardium, both signs of tissue remodeling and scar tissue deposition. Histological images are cross sectional slices capturing the left (larger chamber) and right (smaller chamber) ventricles.
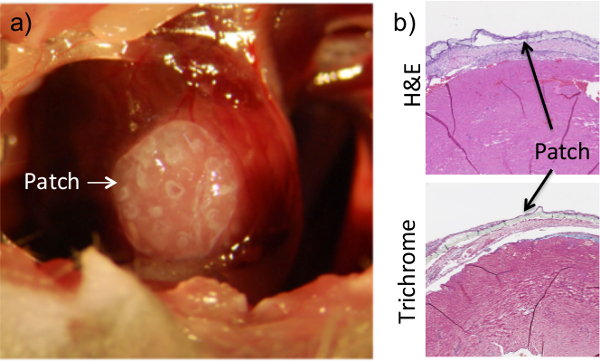
Figure 2: Application of Fibrin Flue Ensures Patch Adhesion to the Heart. The patch is placed on the surface of the heart while the chest cavity is exposed during the procedure (a). Once placed, a fibrin-based glue is added on top of the heart and allowed to dry. The patch can clearly be seen on histological sections of heart tissue that were collected at 1 week post-procedure (b). Dissociation of the patch from the heart surface in histological images is an artifact of the collection and sectioning process. Results are consistent for up to 8 weeks of adhesion.
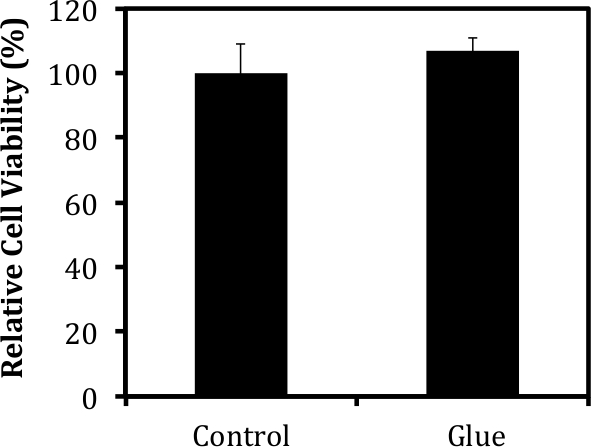
Figure 3: Fibrin-based Glue Does Not Harm Encapsulated Tissues. Cell viability was measured via MTT analysis 1 week after the administration of a fibrin-based glue using protocols described in detail in previous publications8. The viability of cells within the patch was not affected by the addition of the glue to the surface of the construct.
