The “all laser” surgical procedure is proposed to perform minimally invasive corneal transplantation. The procedure is easy to perform (see Figure 1): with respect to a standard endothelial transplant only the steps of measuring the corneal thickness, staining the donor tissue and delivering the laser light are added. The achieved advantages largely compensate an increased surgical time of a few min. The use of intraoperative OCT to measure the donor cornea thickness and the femtosecond laser used to customize the donor lenticule dimensions enables the improvement of the donor/host interface adhesion (see Figure 2). In doing so, the surgery is designed following the needs and morphological characteristics of the single patient. The laser welding procedure provides an immediate closure of the donor/host interfaces4. In a standard technique, it is not possible to suture the donor tissue in any way, because of its biomechanical characteristics and location. The common postoperative risk is the donor lenticule dislocation. In our experience, donor endothelium dislocation did not occur in any of the 15 treated patients. To reach this goal it is important to deliver a complete ring of spots, covering the external diameter of the donor/recipient interface. At the beginning of the clinical trials, we performed a semicircular welding trajectory in selected patients. In one of these patients suffering from Fuch’s dystrophy with corneal deficit, a partial dislocation of the lenticule was observed (see Figure 3): interface adhesion was evident only at the welded site. For this reason, we experimented the procedure delivering a complete ring of spots, with optimized results.
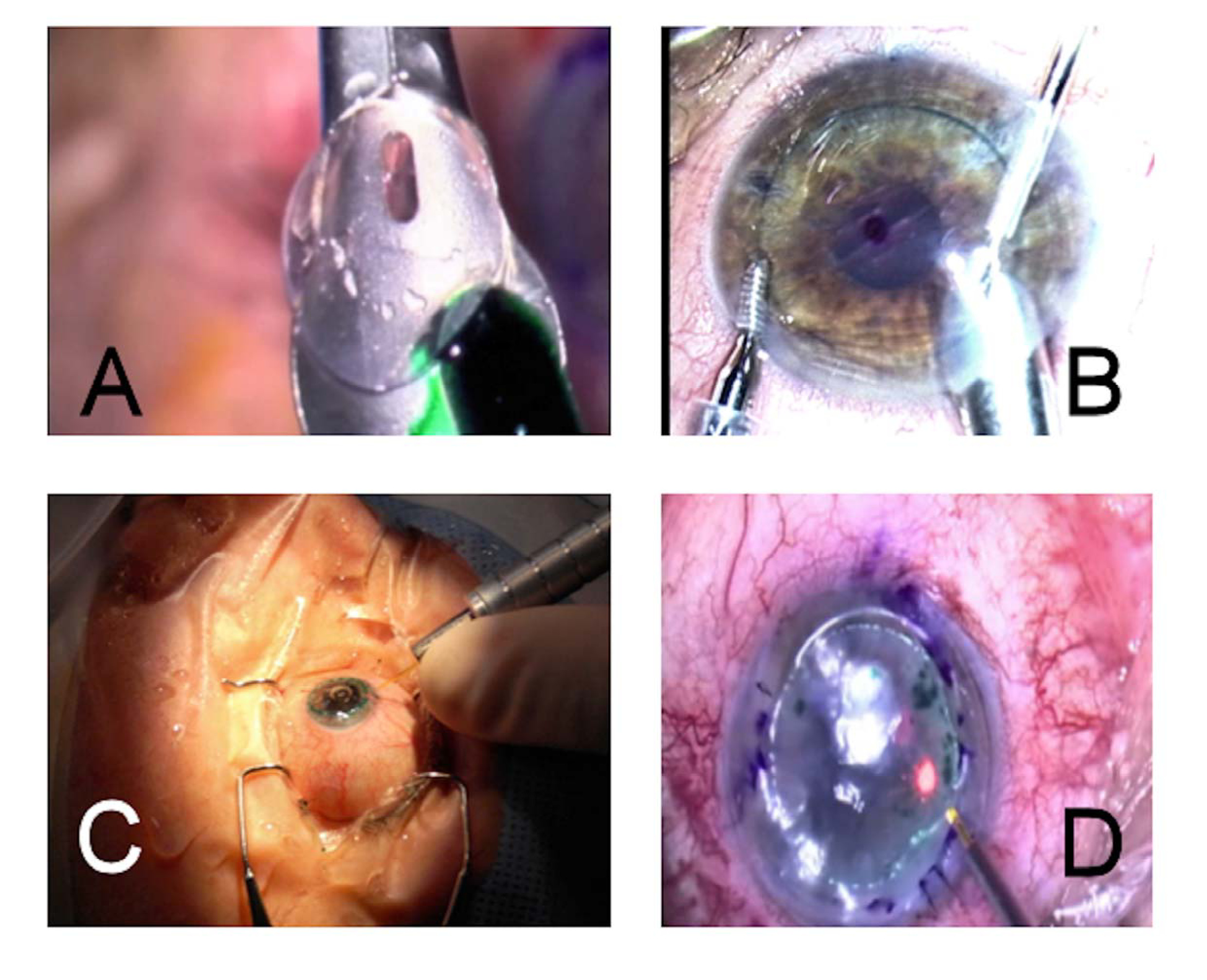
Figure 1: Endothelial Transplant. (A) The donor endothelium is put onto the injector and its inner surface is stained with a water solution of Indocyanine Green. (B) The endothelium is inserted inside the patient’s eye and positioned in its final and correct location. (C and D) Laser welding is provided from the outside, delivering single spots with a 300 µm core diameter optical fiber, mounted on a hand piece.
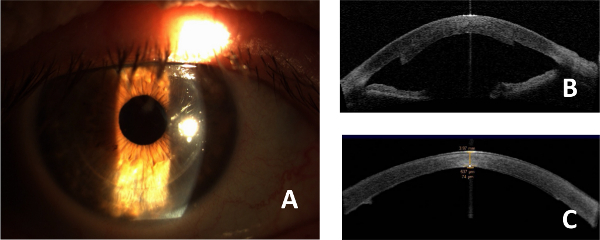
Figure 2: Postoperative results. (A) Slit lamp image of a transplanted eye, 1 week after surgery. No residual ICG is present, photothermal damage at the donor/host interface is not evident. (B) OCT image of a transplanted endothelium with the proposed “all laser” technique and without performing donor cornea thickness measurement (1 week after surgery). The transplanted endothelium is thick, with poor adhesion at the periphery. (C) OCT image of a transplanted endothelium with the proposed “all laser” technique and OCT donor cornea thickness measurement (1 week after surgery). The thickness lenticule is regular and the adhesion is good.
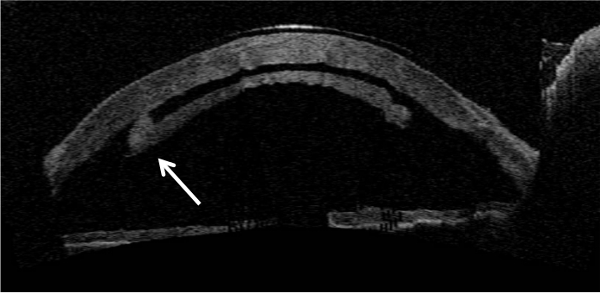
Figure 3: Laser welding efficiency. OCT image of a partially welded endothelium in a patient with Fuch’s dystrophy, 1 day after surgery. In this patient, only a portion of the endothelium was welded onto the recipient’s stroma: donor lenticule dislocation was observed the first day after surgery; this image shows the evidence that the adhesive effect was present only at the weld sites (white arrow).
