The performance of SPRi and Nano-SPRi (SPRi employing the NanoEnhancers) was compared with ELISA for the detection of rhGH in a complex environment. The differences in the setup of these methods are described here briefly. For SPRi (direct detection, Figure 1), the capture antibody is immobilized on the surface and then the sample is injected and binding of analyte to the sensor surface is measured directly in real time and label-free manner. However, with Nano-SPRi (Figure 1), after the analyte binds to the sensor surface, a consecutive injection is followed with quantum dots coated with detection antibodies to amplify the SPRi signal.
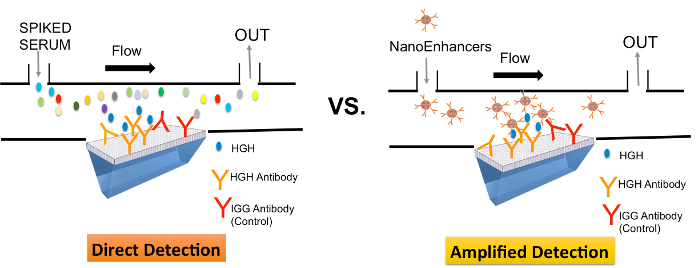
Figure 1. A schematic representation comparing direct-mode (SPRi) and amplified-mode (Nano-SPRi) of detection of rhGH in crude samples. Ligands (rhGH or IgG specific antibodies) were immobilized in an array format on the SPRi biochip. Target protein (rhGh) spiked in human serum introduced to the sensor surface are directly detected (SPRi) and sequentially highlighted with NanoEnhancers (Nano-SPRi). Please click here to view a larger version of this figure.
As for ELISA, the multiwell plates arrive already pre-functionalized with capture antibody and then sample is introduced, the analyte of interest will bind. A detection antibody is introduced followed by substrate addition. The optical density is then measured at 450 nm. In this study, a commercial ELISA kit (Figure 2) was used to measure rhGH spiked in 10% human serum.
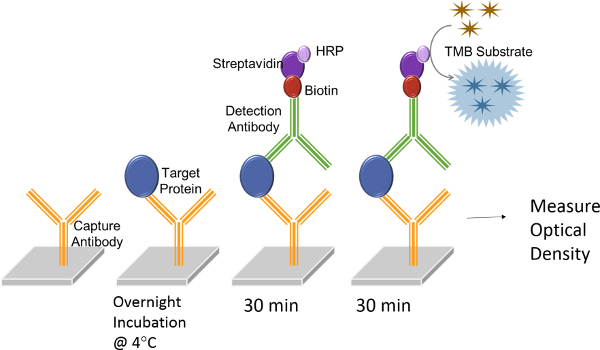
Figure 2. A schematic representation of ELISA assay procedure. rhGH protein (blue ovals) is introduced to wells that have been pre-functionalized with monoclonal antibodies (yellow) specific to rhGH. Non-specific interactions are eliminated by rinsing the wells with wash buffer followed by the introduction of a detection antibody prefunctionalized with horseradish peroxidase (HRP, purple). The solution will change in color after adding the substrate tetramethylbenzidine (TMB, gold). Please click here to view a larger version of this figure.
Figure 3 represents the titration curve of rhGH spiked in 10% human serum and is plotted against the obtained OD at 450 nm. A good linear response was observed and the limit of detection was determined to be 1 ng/ml. The coefficient of variation (CV) was 6.5% suggesting good reproducibility.
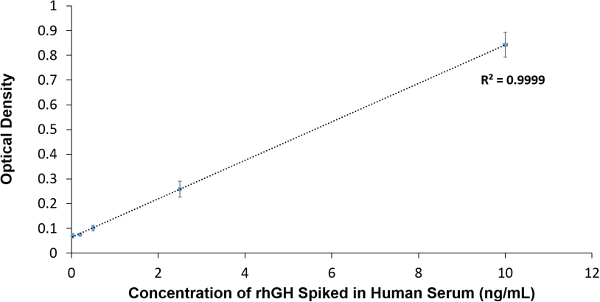
Figure 3. ELISA data Analysis. Concentration of rhGH spiked in serum is plotted against the obtained OD at 450 nm. Please click here to view a larger version of this figure.
Next, the detection of rhGH spiked in human serum was assessed with SPRi. Direct detection of rhGH resulted with the corresponding concentration gradient curve (Figure 4), each point represents the average value of the reflectivity difference calculated from three SPRi kinetic curves for each concentration. The limit of detection (LOD) was determined to be 3.61 ng/ml. The SPRi direct detection assay was highly reproducible as the CV of the assay was only 4.1%.
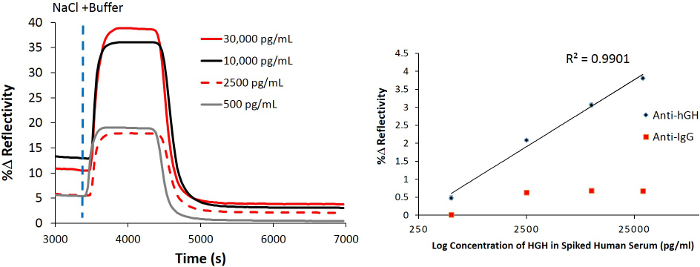
Figure 4. Direct SPRi detection of hGH spiked in 10% human serum. The resultant normalized SPRi kinetic plot after the injection of various amounts of hGH spiked in human serum followed by the injection of a high salt buffer (dashed vertical line) to remove non-specific interactions . A concentration gradient curve representing the binding of various amounts of hGH spiked in human serum to the sensor surface that has been prefunctionalized with biotinylated hGH-specific-Antibody . Please click here to view a larger version of this figure.
To increase the sensitivity of the SPRi biosensor, NanoEnhancers (QDs pre-functionalized with detection antibodies) are sequentially introduced to the sensor surface in order to highlight the presence of rhGH spiked in human serum. After background subtraction, the NanoEnhancers were able to amplify the biosensor response up to 7.9%, however, with minimal signal change (Immunoglobulin G (IgG) -specific antibody, 0.38% change in reflectivity; Figure 5 on controlled regions of interest. Imaging of the sensor surface revealed that only regions of interest that have rhGH-specific antibodies immobilized experience the largest contrast change corroborating directly with the kinetic sensorgram response.
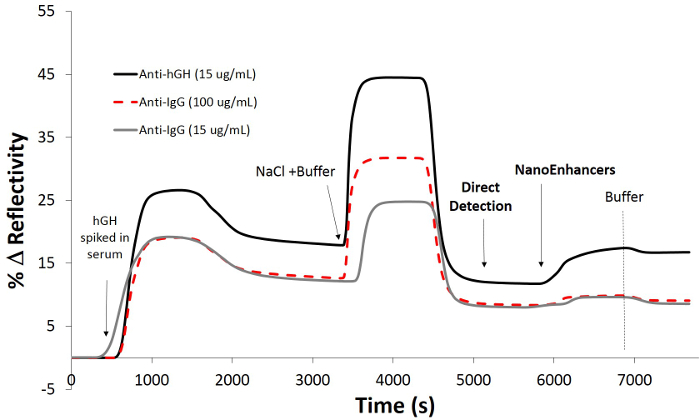
Figure 5. Detection of rhGH using a sandwich assay spiked in 10% human serum. SPRi kinetic plot after the injection of rhGH (30 ng/ml) in buffer (10 mM PBS, 150 mM sodium chloride, pH = 7.4) onto a pre-functionalized chip with 11-mercaptoundecanoic acid / rhGH-specific antibody and control IgG-antibody then blocked with BSA followed by the addition of detection antibody-coated quantum dots (NanoEnhancers). Please click here to view a larger version of this figure.
To demonstrate the practicability of the Nano-SPRi biosensor, the measuring range of rhGH in crude samples was assessed. An extended working range from 30,000 pg/ml to 0.25 pg/ml resulted as a response to the addition of NanoEnhancers (Figure 6). It is worth noting that each point on the titration curve is averaged from three independent experiments. Consequently, the lower limit of detection was calculated to be 9.20 pg/ml and the coefficient of variation was 20%.
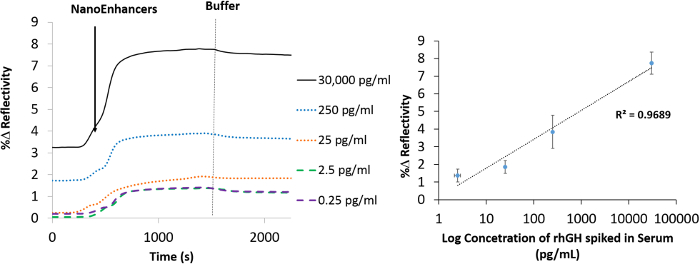
Figure 6. Nano-SPRi detection of hGH spiked in human serum. Normalized SPRi kinetic plot representation of hGH_specific_Anti-QDs-amplified signal for human serum samples spiked with different concentrations of hGH. A vertical dashed line (grey) represents the injection point of the running buffer. (b) A concentration gradient curve representing the binding of NanoEnhancers (hGH_specific_Anti-QDs) after the injection of various amounts of hGH spiked in human serum to the sensor surface that has been prefunctionalized with 11-mercaptoundecanoic acid /hGH-specific antibody. Please click here to view a larger version of this figure.
Next, the change that occurs in the SPR reflectivity curve as a function of the concentration was compared between the direct and the NanoEnhancer bioassay method (Figure 7). For the direct detection technique between 25 and 0.25 pg/ml, the signal started to plateau and this is not surprising as these concentrations fall below the LOD of 3 ng/ml (Figure 7). Similarly, for the amplified technique, concentrations below the LOD of 9.2 pg/ml signal started to plateau and showed virtually no variation.
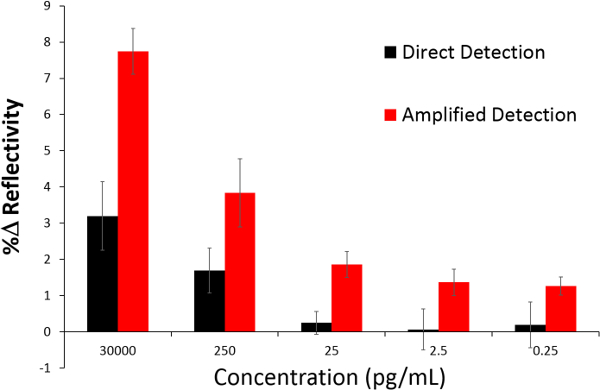
Figure 7. A comparative analysis of SPRi with Nano-SPRi. This bar graph depicts the percent change in reflectivity (%R) after introduction of rhGH spiked in human serum (direct detection) followed by the injection of NanoEnhancers (amplified detection) for 30,000 pg/ml, 250 pg/ml, 25 pg/ml, 2.5 pg/ml and 0.25 pg/ml. Please click here to view a larger version of this figure.
Furthermore, the specificity of the Nano-SPRi biosensor was assessed. Insulin-like growth factor-1 (IGF-1) spiked in human serum was injected as a control since hGH stimulates the secretion of IGF-1 through the growth hormone receptor on the hepatocyte membrane. After the injection of the IGF-1 in serum, the NanoEnhancers were sequentially injected and the SPR signal response did not show any specific binding (Figure 8). However, when rhGH spiked in serum sample was injected to the very same spot functionalized with rhGH antibody, signal enhancement was observed. In conclusion, the Nano-SPRi platform has demonstrated excellent specificity and selectivity for rhGH.
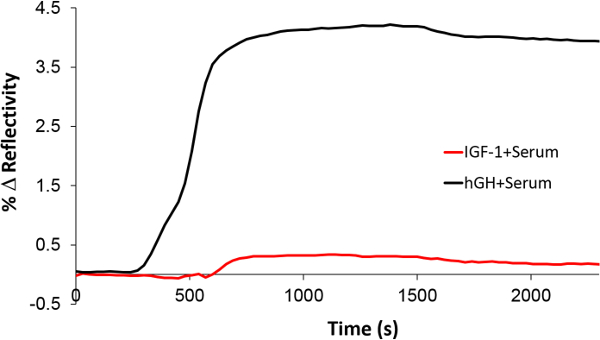
Figure 8. Assessment of Nano-SPRi selectivity towards rhGH. The Nano-SPRi biosensor response after the injection of rhGH (black) and IGF-1 (red) in spiked serum. Please click here to view a larger version of this figure.
A correlation analysis was performed using the Pearson correlation coefficient to determine the correlation between the SPRi signal intensity and ELISA optical density values (Figure 9). A p-value <0.01 was considered significant. As illustrated in this graph, there is a good correlation between the rhGH levels in spiked human serum measured by SPRi and ELISA. The r-value was 0.9263 for 9 different samples.
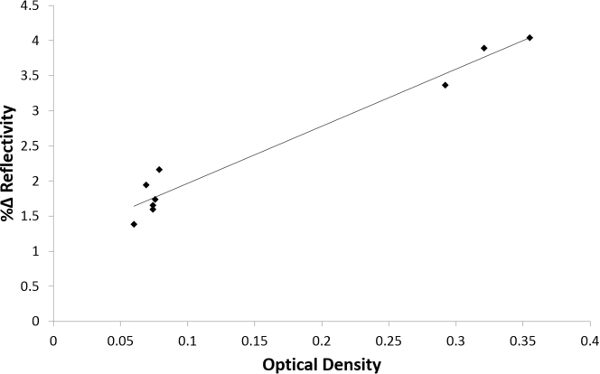
Figure 9. Pearson correlation analysis between ELISA and Nano-SPRi. The plot correlates Nano-SPRi signal intensity (y-axis) with ELISA optical density (x-axis) values. (Pearson correlation coefficient n = 9, r = 0.9263, p = 0.00000183). Please click here to view a larger version of this figure.
The equilibrium dissociation constant (KD) was determined using the graphpad software for ELISA. The calculated KD value was approximately 79 nM (Table 3). The on (Ka) and off (Kd) rates could not be determined by ELISA. However, using the data analysis software, the direct detection method resulted with KD value of 23 pM using the molecular mass of 22 kDa that corresponds to one rhGH molecule. The on and off rates were calculated to be 6.1 x107 M-1s-1 and 1.33 x 10-3 sec-1, respectively. This inherently translates that 0.13% of the rhGH and antibody complexes decay per second. As for the amplified SPRi experiment, a stronger overall interaction was observed between NanoEnhancers and rhGH as the calculated binding affinity was determined to be 4.3 pM. In addition, a stronger association rate was observed for NanoEnhancers and rhGH than capture antibody/rhGH, however the dissociation rate suggests that 0.26% of NanoEnhancer/rhGH/Capture antibody decay per second.
| Method | KD (Affinity) | Ka (on-rate) | Kd (off-rate) | LOD |
| ELISA | 79.45 x 10-9 M | NA | NA | 1 ng/ml |
| SPRi | 23.2 x 10-12 M | 6.1 x 107 M-1sec-1 | 1.33 x10-3 sec-1 | 3.61 ng/ml |
| Nano-SPRi | 4.33 x 10-12 M | 7.54 x108 M-1sec-1 | 2.62 x10-3 sec-1 | 0.0092 ng/ml |
Table 3. Full kinetic data analysis. Evaluation of the affinity, on-rate and off-rate of the antibody responses using graphpad (ELISA) and data analysis (SPRi and Nano-SPRi) software. The determination of the avidity using the molecular mass of 22 kDa that corresponds to one rhGH molecule was chosen. The limits of detection were determined for all three studies using excel.
