The overall time for the surgical procedure was about 30 min from skin incision to wound closure. Using the surgical implants provided, surgery can be performed without a stereo-microscope. Postoperatively, the animals were monitored daily. Post-operative analgesia was terminated after 3 days because none of the animals showed evidence of pain (vocalization, restlessness, lack of mobility, failure to groom, abnormal posture, or lack of normal interest in surroundings) after this time period. The animals showed normal weight-bearing within 2 days after surgery. Wound infection or secondary fractures were not observed during the entire observation period.
The most important complication that can occur is the incorrect implantation of the locking nail, with the protrusion of the nail level with the condyles of the knee joint (Figure 3 A). This mainly occurs due to incorrect handling of the aiming device or due to the use of an animal with a too-small femur, particularly in mice with body weights below 20 g. Another complication is the dislocation of an interlocking pin (Figure 3 B). This complication can be avoided by radiographic confirmation of correct implant placement during or immediately after surgery. This issue is mainly caused by incomplete insertion of the pin. Finally, bone harvest at the end of the experiment was impeded a few times because it was difficult to remove the interlocking pins. This was due to bony bridging around the pin position.
Radiological analyses after 5 weeks confirmed complete healing of the 0.25 mm osteotomy gap. At this time point, the periosteal callus was almost completely remodeled (Figure 4 A). In contrast, in femora stabilized with a 2.00 mm gap, the osteotomy was not healed. The femora reliably showed an atrophic non-union formation. This was also confirmed after 10 weeks of bone healing (Figure 4 B).
After stabilization with a 0.25 mm osteotomy gap, histological analyses revealed a typical pattern of secondary fracture healing with callus formation, including intramembranous and endochondral ossification. After 5 weeks, the osteotomy was completely bridged with osseous tissue. At this time point, woven bone was already remodeled into lamellar bone (Figure 5 A). In contrast, the femora stabilized with 2.00 mm osteotomy gaps showed atrophic non-union after 10 weeks of observation. This was associated with a high amount of fibrous tissue within the osteotomy gap. None of the osteotomies showed signs of bone healing or bridging when analyzed histologically (Figure 5 B).
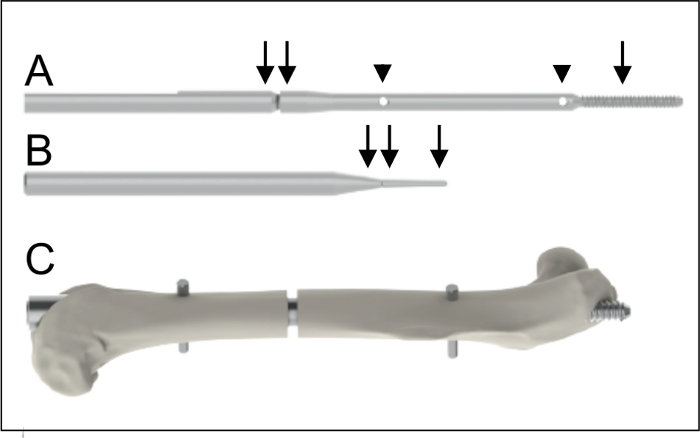
Figure 1: Implants. A. Intramedullary nail (0.8 mm diameter, 15.7 mm length) with a proximal thread (arrow, 4 mm length) and two holes (arrow heads) for the insertion of the interlocking pins. The nail is connected to a shaft (double arrow) to facilitate application. B. Interlocking pin (0.3 mm diameter, arrow) to achieve rotational and axial stability. The interlocking pin is also connected to a shaft (double arrow) to facilitate application. C. Intramedullary nail after implantation into a mouse femur. Please click here to view a larger version of this figure.
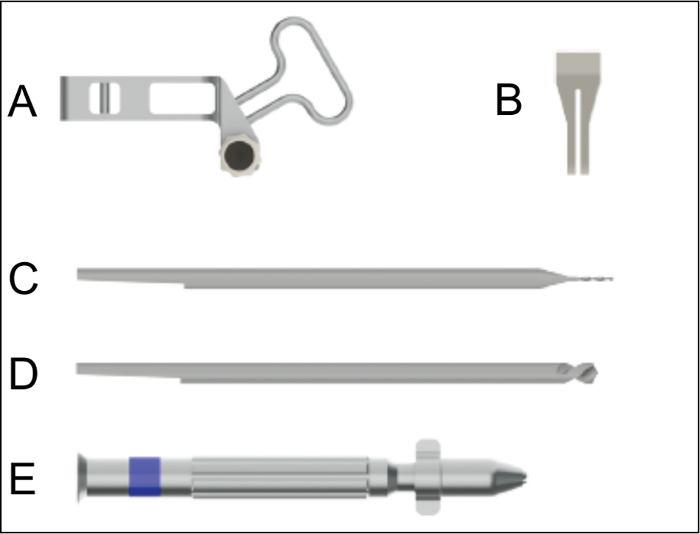
Figure 2: Surgical instruments for nail implantation. A. Aiming device for the insertion of the nail. B. Saw guide to be used for the creation of the osteotomy with a gap size of 0.25 mm. C. Drill bit for drilling the hole for the interlocking pins. D. Centering drill bit for countersinking of the interlocking pin holes. E. Hand drill used for the insertion of the nail, the countersinking, the hole drilling, and the insertion of the interlocking pins. Please click here to view a larger version of this figure.
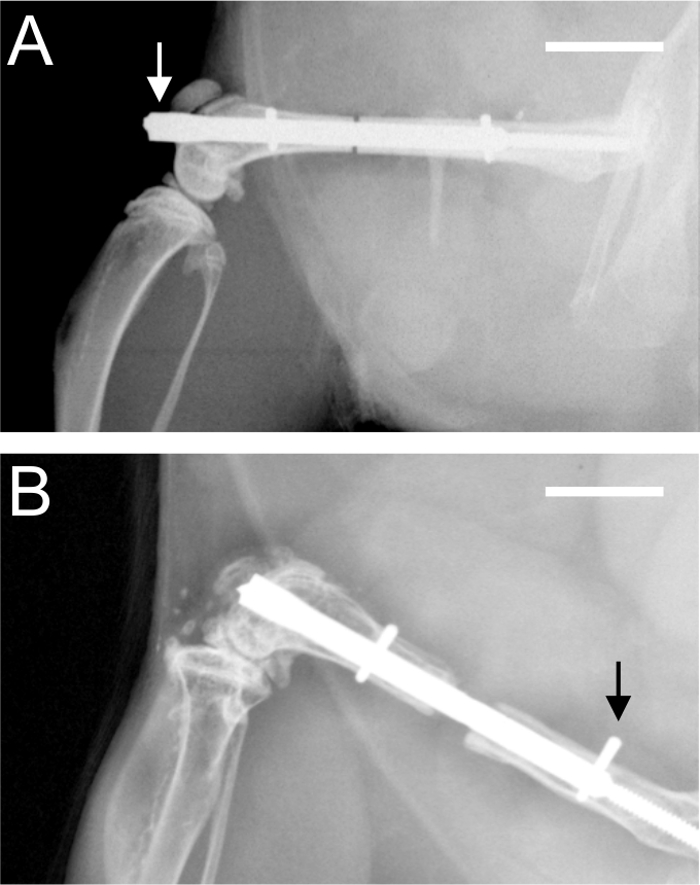
Figure 3: Postoperative radiographs. A. Radiograph demonstrating a protrusion (arrow) of the nail into the knee joint at the level of the condyles. B. Radiograph demonstrating an incomplete insertion of the proximal interlocking pin (arrow). Scale bars represent 4 mm.
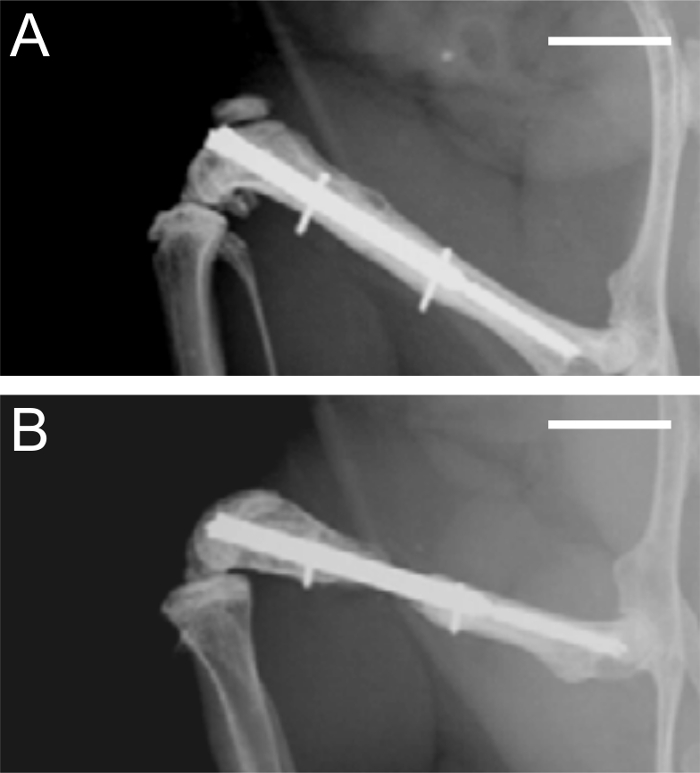
Figure 4: Radiographs after 5 and 10 weeks of bone healing. A. Radiographic analysis of a femur stabilized with a 0.25 mm osteotomy gap after 5 weeks, demonstrating adequate bone healing. B. Radiographic analysis of a femur stabilized with a 2.00 mm osteotomy gap after 10 weeks, demonstrating atrophic non-union. Scale bars represent 4 mm.
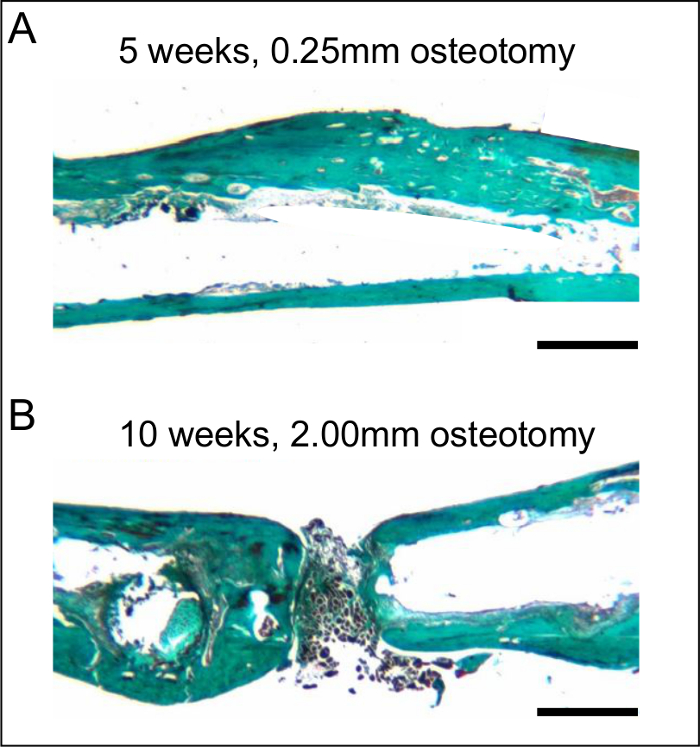
Figure 5: Histological sections after 5 and 10 weeks of bone healing. A. Histological analysis of a femur stabilized with a 0.25 mm osteotomy gap after 5 weeks, demonstrating adequate bone healing. Note the almost-complete remodeling with lamellar bone. B. Histological analysis of a femur stabilized with a 2.00 mm osteotomy gap after 10 weeks, demonstrating atrophic non-union. Note the fibrous tissue in the osteotomy gap. The histological sections were stained according to the trichrome method. Scale bars represent 800 µm.
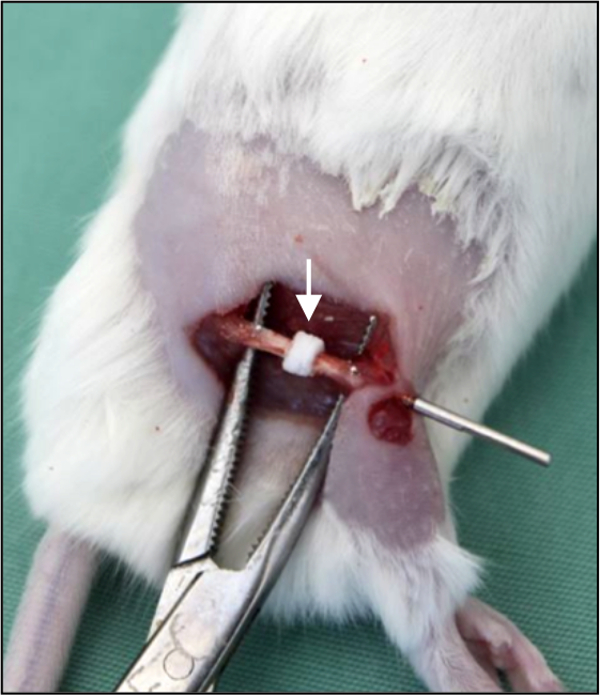
Figure 6: Bone substitute implantation. In vivo photograph demonstrating a segmental bone defect in the right femur of a mouse. The defect is filled by a bone substitute (arrow). The bone substitute is implanted over the nail, providing adequate positioning and fixation.
