This protocol attempted to establish a new cell-based therapy for intractable diabetic wounds. Briefly (as illustrated in Figure 1), allogeneic rASC sheets were created from normal rats using cell-sheet engineering and were then transplanted using a bilayer of artificial skin onto a full-thickness skin defect on a diabetic rat. Light microscope images of a good example of an rASC sheet (Figure 2A) and a bad example of an rASC sheet (Figure 2B) are shown in Figure 2. When ASCs are plated onto a new culture dish, the dish should be slowly rocked back and forth and left and right in an incubator to achieve uniform rASC seeding and a uniformly-thick rASC sheet (Figure 2A). If the rASCs cannot be uniformly attached and cultured on the surface of the culture dish, the sheet cannot be collected as a contiguous ASC sheet (Figure 2B). Figure 3 shows ASC sheets that have been harvested as a contiguous cell sheet at room temperature because the ASCs were uniformly attached to the dish surface. Usually, rASC sheets can be handled with a pair of forceps. If necessary, a transfer membrane can be used to transfer a cell sheet from the culture dish to the wound site, such as if the cell sheet is brittle and fragile.
Figure 4 depicts the ZDF rats used as a diabetic wound-healing model and the transplantation of allogeneic rASC sheets combined with artificial skin. An rASC sheet is soft and flexible, adjustable in size, and capable of being extended to every corner of the wound site with a pair of forceps (Figure 4A-F). The rASC sheet-covered defect was also covered with artificial skin (15 x 10 mm2) and sutured with approximately 10 stitches using a 5-0 nylon suture (Figure 4G). To protect the wound, a moist wound environment was maintained and exudates were absorbed, a non-adhesive dressing (20 x 15 mm2) was placed over the artificial skin, and 5-0 nylon sutures were applied (Figure 4I). The non-adhesive dressing is often removed by the ZDF rats within several days of application. Therefore, the rats must be monitored after transplantation. Usually, the non-adhesive dressing is replaced every 2 days under general anesthesia. Please click here to view a larger version of this figure.
The macroscopic photographs in Figure 5 are the representative results of the transplantation of an rASC sheet. In our previous study, the average wound area in the rASC sheet transplantation group (Figure 5B) was significantly smaller than in the control group (Figure 5A). For the controls, only artificial skin was used to cover the wound, without the transplantation of an rASC sheet. These images were taken on the 14th day after the creation of the wound (n = 6 in each group)31.
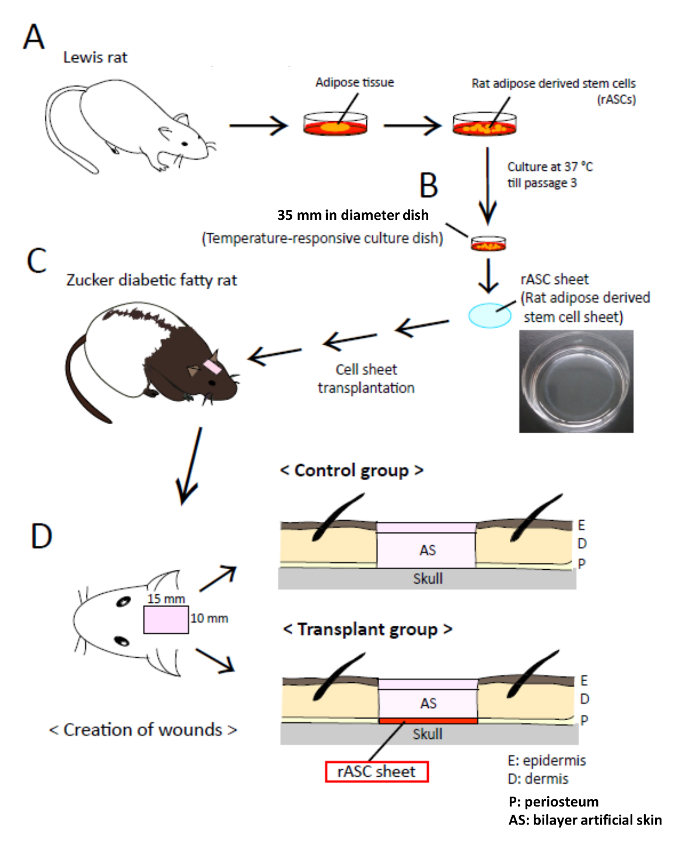
Figure 1: Schematic of the Experimental Transplantation Procedure. Schematic of the experimental transplantation procedure performed with an allogeneic rat adipose-derived stem cell (rASC) sheet and artificial skin in a rat wound-healing model of type 2 diabetes and obesity. (A) Rat adipose tissue was surgically excised from normal Lewis rats. rASCs were isolated and seeded onto a 60 cm2 culture dish and cultured at 37 °C in a 5% CO2 incubator for 7 – 8 days. (B) rASCs were subcultured every 2-3 days, and passage 3 rASCs were seeded onto a 35 mm diameter temperature-responsive culture dish. The cells were cultured in complete medium containing 16.4 µg/mL L-ascorbic acid phosphate magnesium salt n-hydrate (AA) at 37 °C in a 5% CO2 incubator for 7 – 8 days. The rASCs were harvested as a contiguous rASC sheet by reducing the temperature to 20 °C. (C) rASC sheets transplanted onto a 15 x 10 mm2 full-thickness skin defect with exposed bone on the heads of rats exhibiting diabetes and obesity (Zucker diabetic fatty (ZDF) rats) used as a wound-healing model. (D) An rASC sheet was placed on the skull directly over the defect and covered )with a 15 x 10 mm2 sheet of bilayer artificial skin, which was sutured into place with 10 nylon (5-0) sutures. Diabetes 2015;64: 2723-2734; with permission. Diabetes (c) copyright (2015) by the American Diabetes Association. Please click here to view a larger version of this figure.
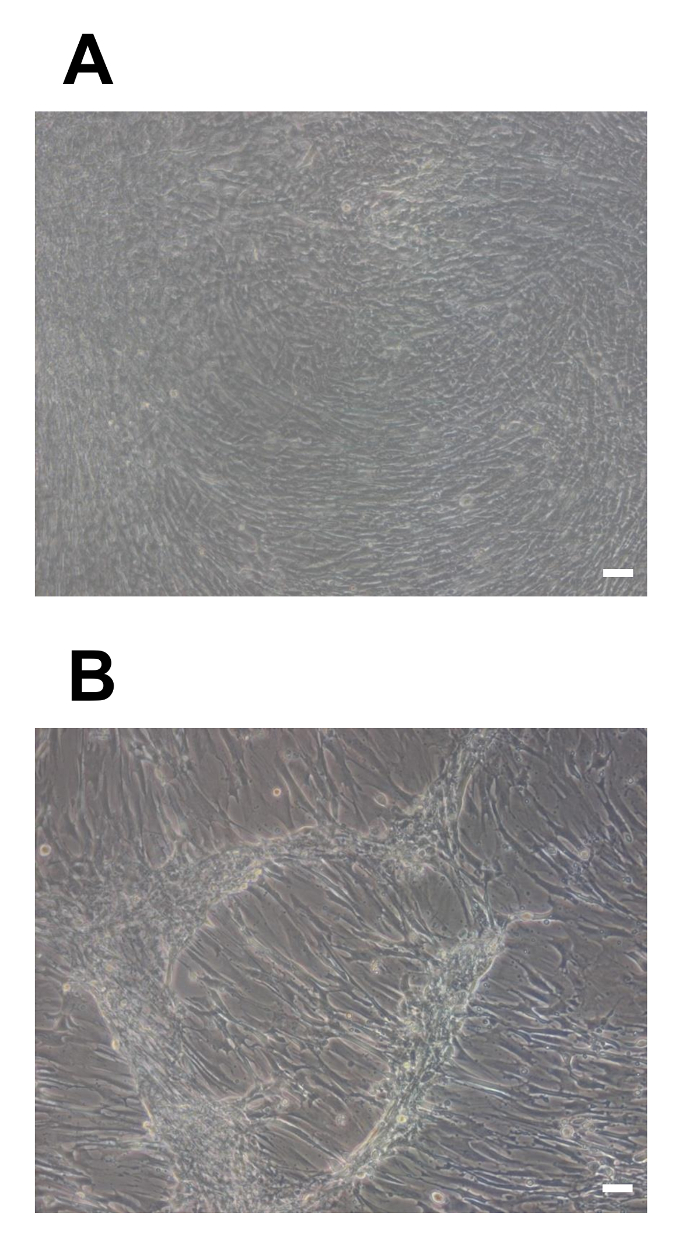
Figure 2: Light Microscope Images of ASCs. Light microscope images of ASC proliferation to the edge of culture dishes, without gaps between the ASCs. (A) An rASC sheet with a uniform thickness in all directions 7 days after the start of culturing (A). (B) An rASC sheet without uniform seeding. A contiguous rASC sheet cannot be obtained on day 7 after the start of culturing (B). Scale bars = 100 µm. Please click here to view a larger version of this figure.
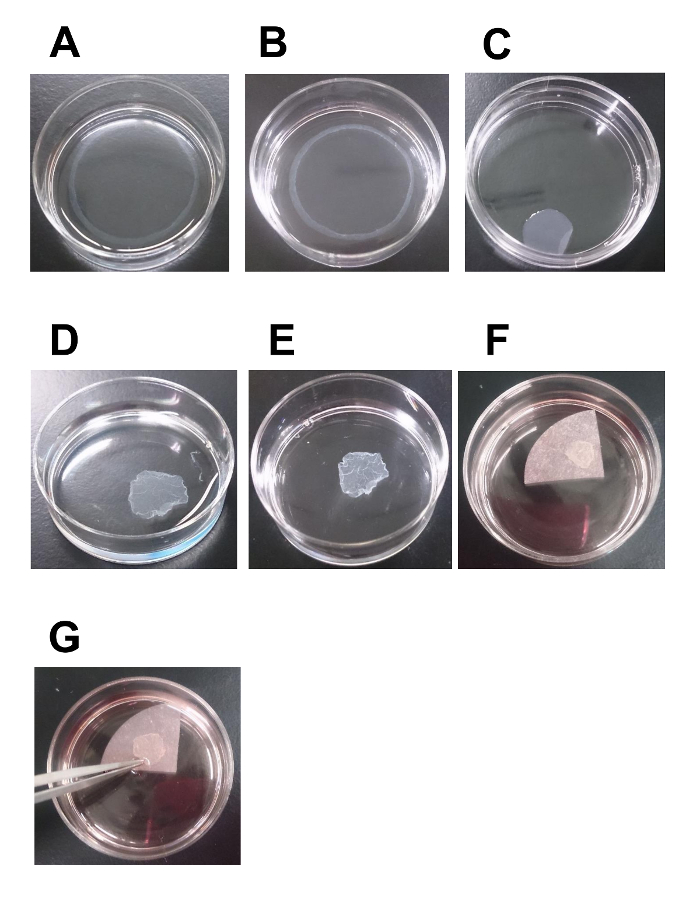
Figure 3: Time-lapse Images of rASC Sheet Statues at Room Temperature. Time-lapse images of the status of an rASC sheet at room temperature. rASCs on a 35 mm diameter temperature-responsive culture dish spontaneously and gradually detached from the dish surface at room temperature (approximately 20 °C) and were harvested as a contiguous sheet. (A) Approximately 5 min after moving the temperature-responsive culture dish to room temperature. (B) Approximately 10 min after moving the 35 mm diameter temperature-responsive culture dish to room temperature.(C) Approximately 20 – 30 min after moving the temperature-responsive culture dish to room temperature. This is a good-quality rASC sheet (C). (D-E) rASC sheet status approximately 20 – 30 min after moving the temperature-responsive culture dish to room temperature. This rASC sheet is of average quality (D). (F-G) rASC sheets are usually handled with a pair of forceps. If the cell sheet is brittle and fragile, a membrane can be used as a scaffold for transferring the cell sheet from the culture dish to the wound site. Please click here to view a larger version of this figure.
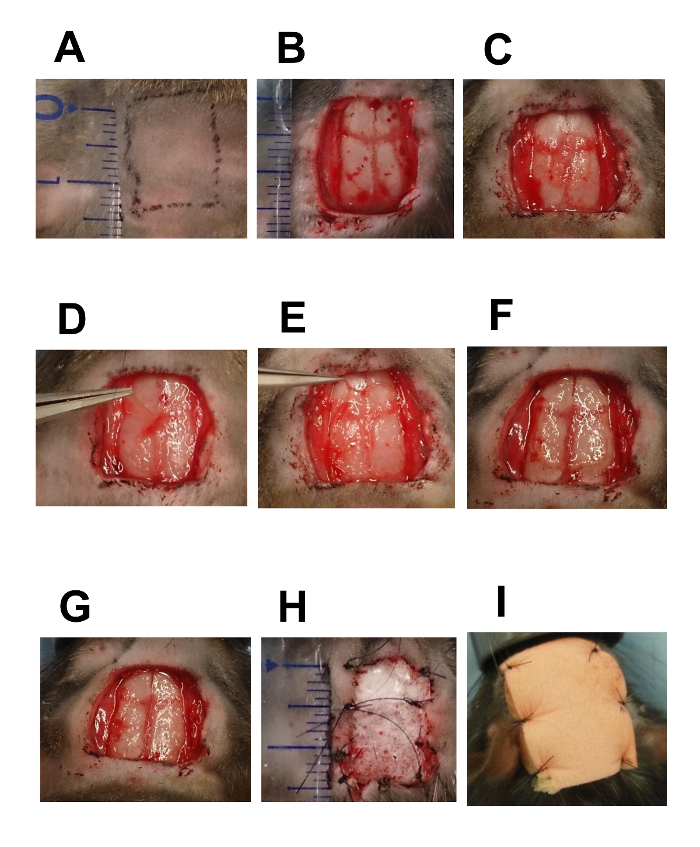
Figure 4: Time-series Images of Wound Creation and rASC Sheet Transplantation with Artificial Skin and a Non-adhesive Dressing
Time series images of wound creation and rASC sheet transplantation with artificial skin and a non-adhesive dressing. (A) The heads of ZDF rats were shaved with an electric razor. After shaving the body hair, check marks (15 x 10 mm2) were drawn using an oily hydrophobic pen. (B) A full-thickness skin defect (15 x 10 mm2) was created on the head of an anesthetized ZDF rat by removing cutaneous tissue from the epidermis to the periosteum. The skin and cutaneous tissue were excised with a scalpel, and the periosteum was removed with a periosteal raspatory. Using gauze moistened with sterile saline, pressure was applied to stop the bleeding after excision. (C) rASC sheet transplantation. An rASC sheet was placed over the defect immediately above the skull of the rat using a pair of forceps. (D-G) Adjusting rASC sheet extension to match wound size. The rASC sheet is flexible, adjustable, and can be extended to every corner of the wound site using a pair of forceps. For wider wounds, two or three flexible rASC sheets can be stacked. (H) Suturing the artificial skin covering the rASC sheet. The defect and the transplanted rASC sheet were covered with artificial skin (15 x 10 mm2), which was sutured with 10 stitches using 5-0 nylon sutures. (I) Suturing of the non-adhesive dressing (20 x 15 mm2) to the wound site covered with artificial skin. To protect the wound, non-adhesive dressing (20 x 15 mm2) was placed over the artificial skin with 5-0 nylon sutures. Diabetes 2015;64: 2723-2734; with permission. Diabetes (c) copyright (2015) by the American Diabetes Association. Please click here to view a larger version of this figure.
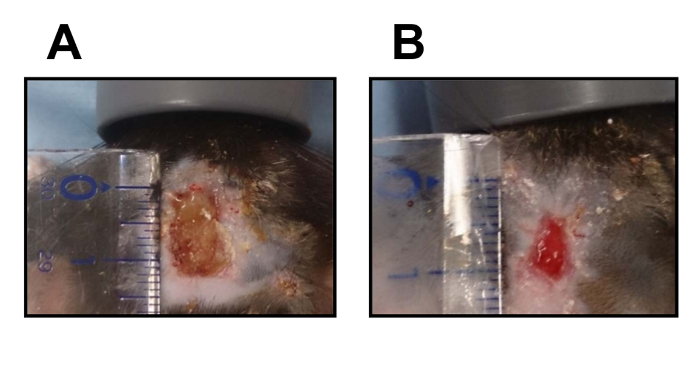
Figure 5: Macroscopic Images of Full-thickness Skin Defects. Macroscopic photographs of full-thickness skin defects without the transplantation of an rASC sheet (A) and with the transplantation of an rASC sheet (B) 14 days after creation of the wound. Please click here to view a larger version of this figure.
