After the patch angioplasty, there was no thrombosis in either the venous (n = 42) or arterial (n = 24) patch groups. Survival at day 7 was 100% in both groups with either a venous or arterial patch.
The patches were harvested on day 7 and stained with hematoxylin and eosin, and the neointimal thickness was compared as previously described7. Because of the distinct morphological difference between the patch and the neointima, it is very easy to discriminate the neointima. In the venous patch, there was a distinct layer of thick neointima on the luminal side of the patch, with more cells accumulated in the neointima (Figure 2A, 2C); in the arterial patch, there was a much thinner neointimal layer, with only a few cells attached to the luminal side of the patch (Figure 2B, 2D). The neointima was significantly thicker in the venous patch compared to the artery patch (Figure 2E). Similar results were obtained on day 14 (data not shown). These results show that the patch venoplasty model is superior over other models to acquire a thick neointima in a short period of time.
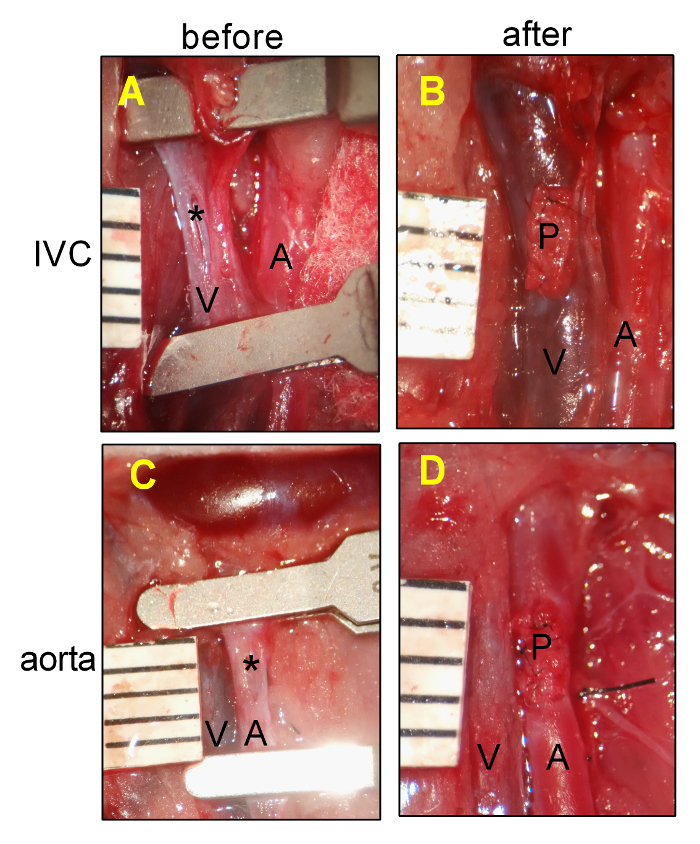
Figure 1: Rat Pericardial Patch Angioplasty. (A) Representative photograph showing the IVC venotomy. (B) Representative photograph showing the IVC after patch placement. (C) Representative photograph showing the aortic arteriotomy. (D) Representative photograph showing the aorta after patch placement. A, aorta; IVC, inferior vena cava; P, pericardial patch; *, posterior intima of IVC or aorta; ruler markings are 1 mm. Please click here to view a larger version of this figure.
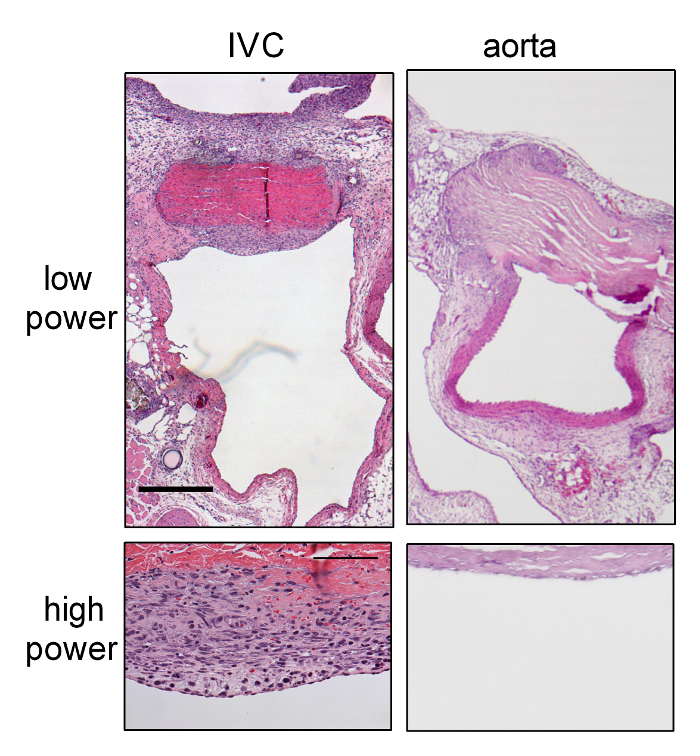
Figure 2: Aggressive Neointimal Hyperplasia in Patch Venoplasty Compared to Patch Arterioplasty at Day 7.
(A) Representative lower-power photograph showing the patch venoplasty on day 7, which was stained with H&E. (B) Representative lower-power photograph showing the patch angioplasty at day 7, which was stained with H&E. (C) Representative high-power photograph showing the neointimal formation on the patch venoplasty. (D) Representative high-power photograph showing the neointimal formation on the patch arterioplasty. Scale bar = 0.5 mm; high power = 100 µm. P, patch; L, IVC or aorta lumen; N, neointima. (E) Bar graph showing increased neointimal thickness in the venoplasty compared to arterioplasty. The error bar denotes the SEM; *P = 0.0015, t-test; n = 4. Please click here to view a larger version of this figure.
