To verify success regarding the establishment of a secondary injury model with the new operative approach using SSAI (Figure 2A), RGCs were retrogradely labeled immediately after model establishment. The purpose of this procedure was to label RGCs retrogradely by injecting a neural tracer dye (3% fluorophore (e.g., Fluorogold) in sterile phosphate buffer saline) into the superior colliculus (Figure 2B). This approach yields reproducible labeling of viable RGCs with little variation.14,15,16,17,18 The dye will be retrogradely taken up by RGCs in the retina and constitutes a marker for live RGCs, with the axons not transected in the right eye. Meanwhile, RGCs corresponding to the partially transected optic nerve axons in the right eye could not be labeled with tracer dye (Figure 2C). As a control eye, the left eye without operation, RGCs along the optic nerve of the retina were all labeled with the fluorescent gold dye in a retrograde manner from the superior colliculus (Figure 2D).
Seven days after partial optic nerve transection and retrograde labeling of RGCs, the retinas were harvested, fixed, flattened, and mounted. The labeled RGCs were imaged under a fluorescent microscope in defined regions of the retina. The results of fluorescence-labeled RGCs with or without partial optic nerve transection are shown in Figure 3. Only the RGCs in the right retina corresponding to the untransected portion of the optic nerve were labeled with fluorescent gold, and a clear boundary of unlabeled and labeled RGCs could be visualized (Figure 3A, Figure 3B), demonstrating the partial transaction of the optic nerve. As a control eye, all RGCs of the left eye retina showed fluorescence (Figure 3C, Figure 3D).
To assess whether the vasculature around the optic nerve head and the ophthalmic artery that supplies blood to the entoretina were injured and affected during the operation, the right eye fundus was imaged before and after surgery. The images showed blood supply to the right eye (operative eye) before and 1 hour after operation. Blood in the arteries was adequate. No obstruction of the vein was observed. These findings indicated that there was no damage to the blood supply system during the operation (Figure 4A, Figure 4B). Therefore, the secondary degeneration model of RGCs was successfully established.
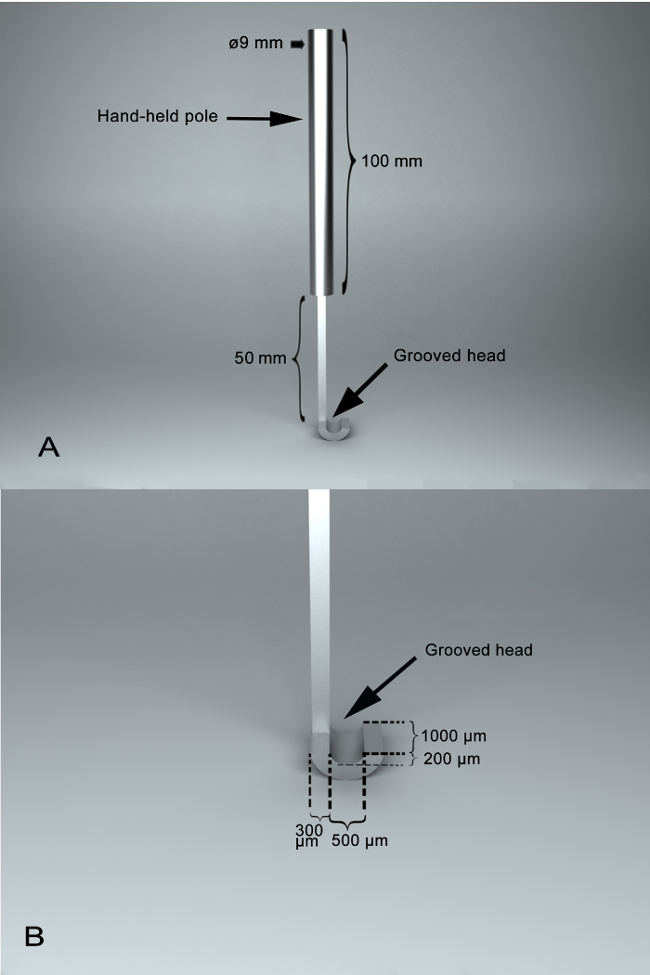
Figure 1: Photographs of self-designed surgical assistant instrument, SSAI. (A) A panoramic view of the surgical instrument,with two main parts, including a hand-held pole and a grooved head. Between them, there is a joint section with a length of 50 mm. The length of the hand-held pole is 100 mm, and the diameter of the hand-held pole is 9 mm. (B) A feature of the SSAI groove. The grooved surface of the grooved head is semi-circular, which enables the optic nerve to lay within it, being stabilized for transection. The grooved surface is with a vertical depth of 200 µm and a width of 500 µm and a length of 1,000 µm. The width of edge of the grooved head is 300 µm. Please click here to view a larger version of this figure.
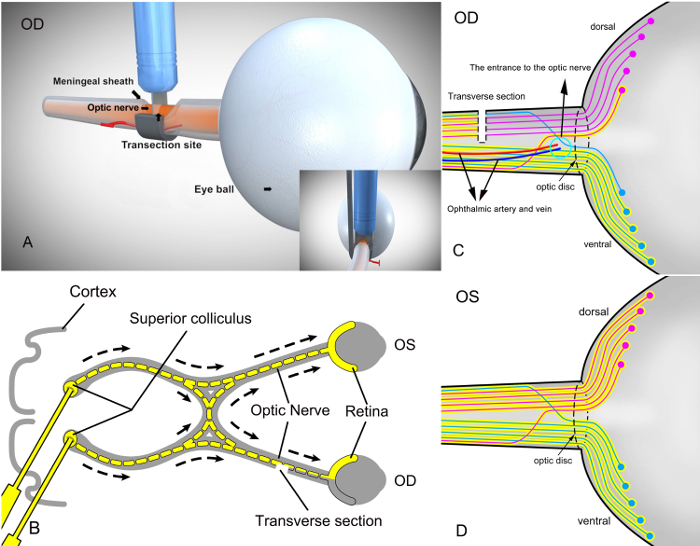
Figure 2: Schematic diagram of RGC labeling on the retina after partial transection of the right optic nerve with the self-designed surgical assistant instrument (SSAI) and retrogradely labeling the superior colliculus with the fluorophore. (A) The surgical view of partial right optic nerve transection in rats with the self-designed surgical assistant instrument (SSAI). (B) After modeling, RGCs were labeled retrogradely by injecting a neural tracer dye (yellow color, 3% fluorophore in sterile phosphate buffer saline) into the superior colliculus in the brain. Since the axons of RGCs reside in the superior colliculus, the tracer dye is taken up by RGCs retrogradely and constitutes a marker for live cells. The transverse section in the figure represents a cross-section of the optic nerve. OD, operated eye; OS, control eye without operation. In (C), only the RGCs corresponding to the untransected portion of the optic nerve were labeled with fluorophore. Blue represents unseparated ventral optic nerves and the corresponding RGCs on the retina; red reflects partially transected dorsal optic nerves and the corresponding RGCs on the retina. (D) The retinal RGCs of the left eye (control eye) without the surgical procedure were all labeled by the dye. Dorsal and ventral optic nerves were all labeled by the dye as well. Please click here to view a larger version of this figure.
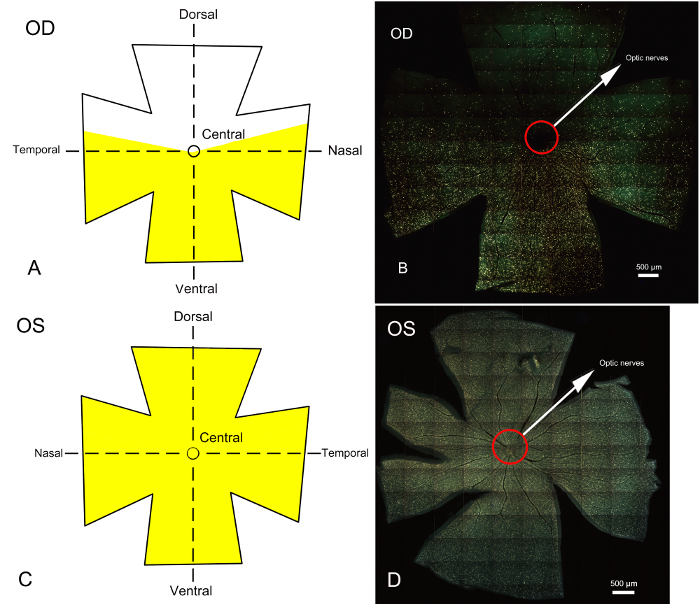
Figure 3: Whole retina epifluorescence micrographs of fluorophore labeled RGCs 7 days after establishing the partial optic nerve transection model and retrograde labeling of the superior colliculus. The corresponding schematic diagrams of Fluorogold stained RGC areas on the retina are also presented. (A) and (C) represent the schematic diagrams of RGCs in the retina of the right (operative) and left (control) eyes after labeling with fluorophore, respectively. Yellow indicates the area labeled with the fluorescent gold dye. The retina is divided into dorsal, ventral and central parts. (B) and (D) represent whole retinal epifluorescence micrographs obtained under a fluorescence microscope; yellow represents the area of RGCs labeled with fluorophore. In the surgical eye (right eye) shown in B, the unlabeled region represents the area of RGCs corresponding to the optic nerve which is partially transected, mainly on the dorsal side of the retina. The region labeled by the fluorescent gold dye is the area of RGCs corresponding to the optic nerve which is not transected and mainly concentrated in the central and ventral sides of the retina. The boundary between the areas of unlabeled and labeled RGCs is clear. Primary degeneration of RGC bodies would be limited to the dorsal retina, and all loss of RGC bodies in the central and ventral retinas could be attributed to secondary degeneration. (D) Whole retinal photomicrograph of the left eye after labeling of RGCs with fluorophore. The RGCs of the left control eye without surgical procedure were totally stained by fluorophore. Scale bars = 500 µm. Please click here to view a larger version of this figure.
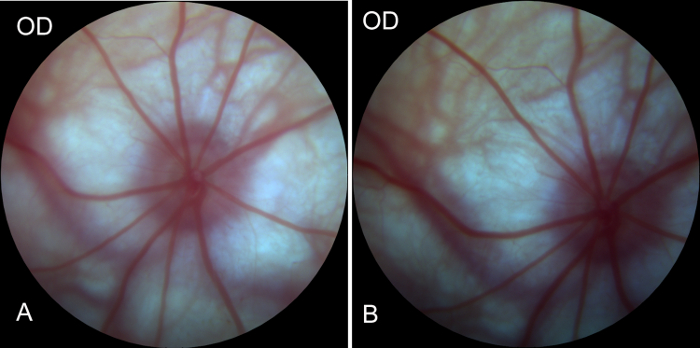
Figure 4: Preoperative and postoperative images of the fundus of the right eye obtained by Fundus camera. (A) Image of the fundus before right eye surgery in rats, showing good blood supply of the fundus, arterial filling, and no venous return or obstruction, indicating a good retinal blood supply system. (B) Image of the fundus of the right eye 1 hour after surgery. Compared with the preoperative image of the fundus, no significant changes were observed in retinal blood supply, indicating that the blood supply system of the eyeball was not affected during the process of modeling. Please click here to view a larger version of this figure.
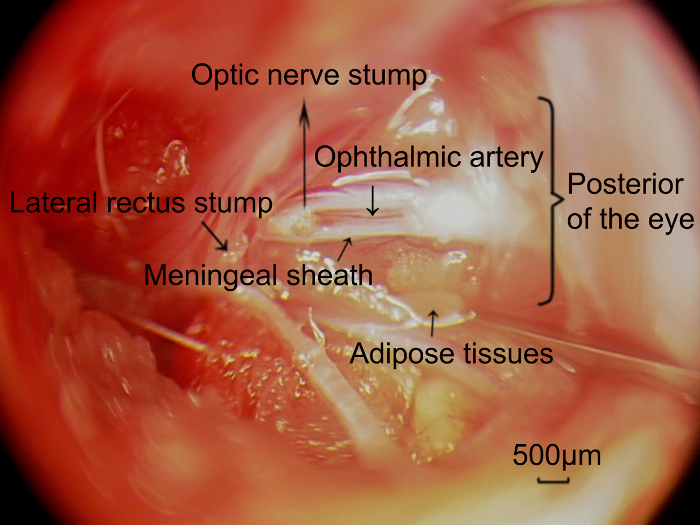
Figure 5: Photographs of the retrobulbar optic nerve and the ophthalmic artery located on the meningeal sheath, captured through the surgical approach. After completely removing the targeted length of the optic nerve, the ophthalmic artery (arrowhead) concomitant with the meningeal sheath of the optic nerve was exposed, and parallel to the optic nerve. Scale bars = 500 µm. Please click here to view a larger version of this figure.
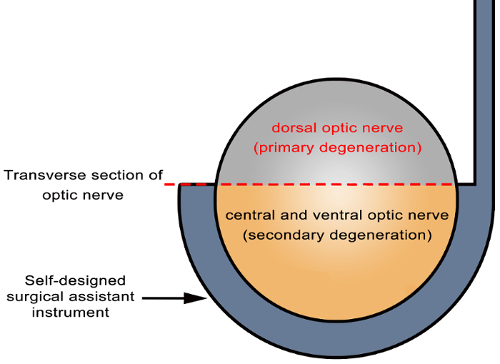
Figure 6: Schematic diagram of primary and secondary degeneration locations in the optic nerve. Partial incision of the optic nerve was achieved using the self-designed surgical assistant instrument (arrowhead). The axons in directly damaged sites (dorsal cutting site of the optic nerve in the transverse section in gray) undergo primary degeneration, while those in indirectly damaged sites (central and ventral areas of the optic nerve in the transverse section in yellow) undergo secondary degeneration. Please click here to view a larger version of this figure.
