The purpose of the orthotopic model is to mimic human cancer progression (i.e., the growth of the primary tumor followed by lymph node metastasis and then distant lung metastasis)15. After cancer cell inoculation, the bioluminescence is quantified regularly (two to three times/week) (Figure 1A). The bioluminescence in the lungs is deeper and smaller than the primary lesion. The bioluminescence mainly reflects the primary tumor burden in live mice3 (Figure 1B and 1C). The tumor size was also measured by caliper measurement. The tumor volume was estimated using the following equation: volume = (length) x (width)2/2 (Figure 1D). Quantification of the tumor burden by bioluminescence and caliper measurement showed similar trends in the representative results (Figure 1B and 1D); however, we sometimes encountered discrepancies. We assume that quantifying the primary tumor burden utilizing bioluminescence is more accurate compared to measuring the tumor size by caliper when the tumor size is less than 1.5 cm. Because it reflects viable cancer cells, even a small number of cells can be detected by bioluminescence, and only cancer cells can be detected inside of the tumor, not including infiltrating immune cells or surrounding stromal cells3. This model is useful in evaluating the efficacy of tumor regression mediated by anti-cancer drug and immune responses3,7,16. The tumor burden of the lung metastases can also be quantified by ex vivo imaging in this model (Figure 1E); however, the limitation is that the mice must be euthanized to quantify the metastatic tumor burden.
The purpose of the mastectomy model is to 1) reproduce the standard of care treatment of human breast cancer, which is the surgical removal of the primary tumor17, and 2) allow the serial quantification of the metastatic tumor burden in vivo. This model is particularly useful in the preclinical study of the development of novel therapeutics13. As previously published, an Src inhibitor, AZD0530, which showed efficacy in the preclinical mice model but failed in a clinical trial for breast cancer treatment, showed efficacy in the primary lesion utilizing orthotopic inoculation without mastectomy but not in lung metastasis utilizing the mastectomy model presented here. Although anti-cancer drugs (e.g., anthracyclines) are sometimes used in humans as neoadjuvant therapy to treat primary breast tumors, the vast majority of drugs are used as adjuvant therapy where drugs are given after surgery to reduce the risk of recurrence by treating clinically undetectable cancer or as palliative treatment for metastatic cancer1,7,18. Thus, this mastectomy model was established, which mimics the human treatment process11.
Eight days after the cancer cell inoculation, the primary tumor is surgically removed (Figure 2). To test any of the drug efficacies for metastatic lesions, it should be administrated after the mastectomy. This model allows for lung metastatic lesion quantification, as well as whole-body metastatic lesion quantification, as long as the metastatic tumor burden has a detectable bioluminescence utilizing in vivo imaging. The anterior chest wall local recurrence rate is quite low. In our experience, the local recurrence rate was less than 5% in over 50 mice experiments. However, if the postoperative day 1 bioluminescence exceeds 1.00E + 06 photons (10x larger than other individuals), there is a high possibility of a local residual tumor13. If there are remnant cancer cells present, a palpable tumor appears within two weeks. When there is a local residual tumor, the bioluminescence mainly reflects that local recurrence rather than any metastatic lesions. Local residual tumors are known to behave very differently than distant metastases19; thus, those animals with local recurrence (<5% in our experience) should be excluded from any further analysis. This mastectomy model also allows for serial metastatic tumor burden monitoring without having to euthanize the animals. Furthermore, such bioluminescent monitoring can be confirmed by ex vivo lung metastasis quantification. Instead of quantifying lung metastases by ex vivo imaging, thus having to euthanize the animals, mice survival after surgical treatment can also be monitored as a translatable clinical endpoint (Figure 2D). Since there is no primary lesion, mice cannot meet euthanasia tumor criteria which are generally defined as a tumor size of >2 cm or ulceration of the primary tumor. In this 4T1 mastectomy model, all mice died within 60 days after cancer cell inoculation due to metastasis.
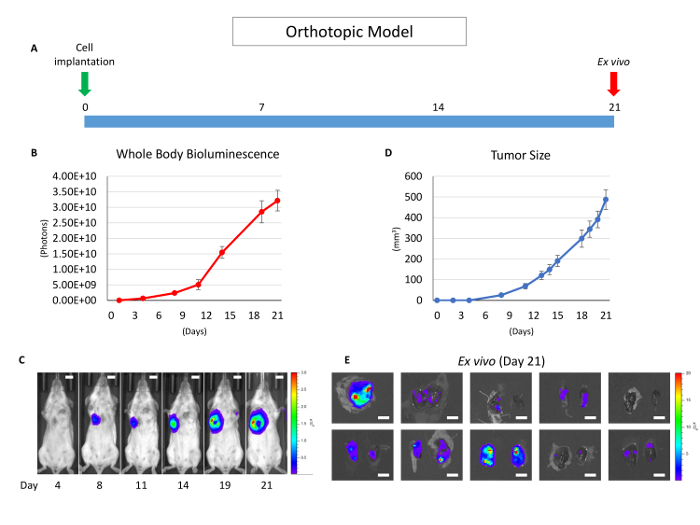
Figure 1: Overview of the orthotopic model without mastectomy. (A) This panel shows a time course of the orthotopic model utilizing the 4T1 syngeneic model. (B) This panel shows the whole-body bioluminescence of an orthotopic model which mainly reflects the primary tumor. The error bar indicates the standard error of the mean (n = 10). (C) This panel shows serial images of whole-body bioluminescence (of the same mouse). The scale bar indicates 1 cm. (D) This panel shows the actual tumor size of panel B, measured by calipers. The error bar indicates the standard error of the mean (n = 10). (E) This panel shows lung ex vivo bioluminescence images of 10 orthotopic model mice (n = 10). The scale bar indicates 1 cm. Please click here to view a larger version of this figure.
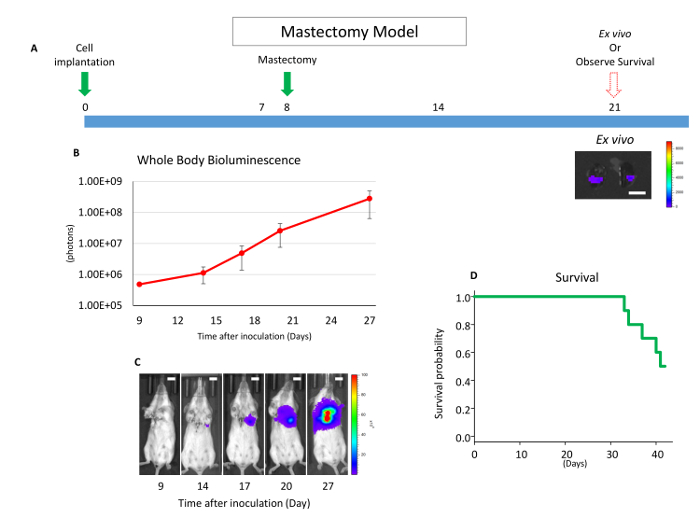
Figure 2: Overview of the mastectomy model. (A) This panel shows a time course of the mastectomy model after 4T1 orthotopic syngeneic implantation. The scale bar indicates 1 cm. (B) This panel shows the whole-body bioluminescence of the mastectomy model, which mainly reflects metastatic lesion. The error bar indicates the standard error of the mean (n = 10). (C) This panel shows serial images of whole-body bioluminescence (of the same mouse). Utilizing ex vivo imaging, it was confirmed that the signals were from lung metastasis, and no local recurrence was confirmed by whole-body imaging after lung removal. Scale bar = 1 cm. (D) This panel shows the Kaplan-Meier survival curve of the mastectomy model without any drug treatment. Mice were euthanized when they reached euthanasia criteria with any morbid condition. Please click here to view a larger version of this figure.
