We analyzed a panel of angiogenesis-related circulating miRNAs in relation to progression-free survival (PFS), overall survival (OS) and objective response rate (ORR) in a 52 mCRC patients treated with B-based CT. The evaluation of such biomarkers in plasma samples is challenging because of technical difficulties. We used established methods for miRNA extraction from patient plasma samples, reverse transcription and pre-amplification. Following the manufacturer's instructions and with only a few modifications required, especially in the extraction steps, we successfully evaluated all our targets in the patient population (Figure 2).
In particular, we analyzed 2 plasma samples/patient, correlating baseline and therapy-modified miRNA expression with patient outcome.
We performed serial dilutions of cel-miR-39 at 0.05 nM, 0.5 nM, 5nM and 5 pM in 800 µL of plasma sample (400 µL of plasma plus 400 µL of 2x denaturating solution) to determine the spike-in concentration to use. As shown in Figure 4, the exogenous control showed threshold cycle (Ct) values that were congruent with the serial dilutions, indicating the robustness of the entire protocol (i.e., extraction, reverse transcription and qRT-PCR evaluation). Moreover, these serial dilutions enabled us to select the spike-in concentration that would not interfere with the reverse-transcription of all target miRNAs.
This method allowed us to correlate baseline miRNAs with clinical pathological features. In particular, we found that hsa-miR-199a-5p, hsa-miR-335-5p and hsa-miR-520d-3p were significantly upregulated in left-sided with respect to right-sided lesions (p = 0.03, p = 0.006 and p = 0.008, respectively). Conversely, hsa-miR-21-5p was significantly downregulated in RAS-mutated patients (K-RAS, p = 0.01 and N-RAS, p = 0.008), whereas hsa-miR-221-3p was upregulated (p = 0.05, p = 0.01, K- and N-RAS, respectively).
Comparing the expression levels of miRNA between baseline and first clinical evaluation, we observed that an increase in hsa-miR-155-5p expression levels was associated with shorter PFS (p = 0.04) and OS (p = 0.02). In particular, in patients with a ≥30% increase in hsa-miR-155-5p, PFS was 9.5 months (95% CI, 6.8-18.7) and OS was 15.9 months (95% CI, 8.4-not reached) compared to 22.3 months (95% CI, 10.2-25.5) and 42.9 months (95% CI, 24.8-not reached) for those with a <30% increase (Figure 3). The median value of variation in the case series (30%) was set as the cutoff point. Circulating basal levels of miRNAs were dichotomized into "high" or "low" according to median values9.
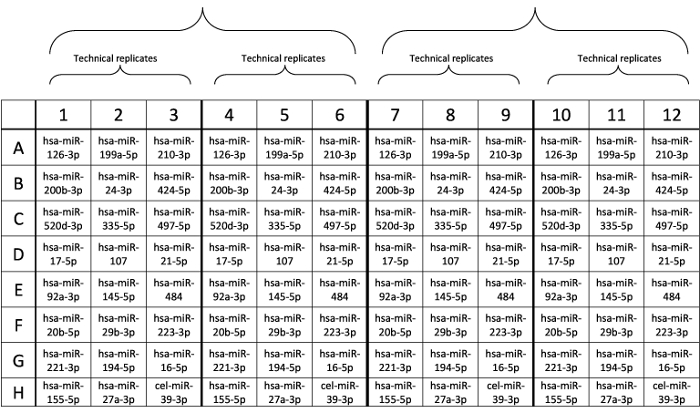
Figure 1: Design of custom plate layout. Probes were pre-spotted in each well. Please click here to view a larger version of this figure.
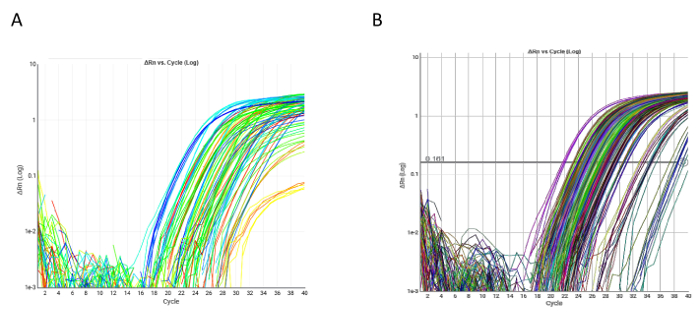
Figure 2: Examples of qRT-PCR amplification plots. (A) Amplification plot of a single qRT-PCR custom plate. All markers were evaluable in both single plate samples. (B) qRT-PCR of hsa-miR-17-5p in the overall case series. Please click here to view a larger version of this figure.
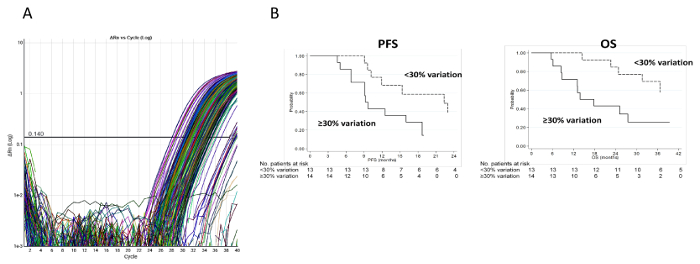
Figure 3: Experimental and clinical results relative to hsa-miR-155-5p. (A) Ct values for hsa-miR-155-5p. Amplification plot of hsa-miR-155-5p in the overall case series. (B) PFS and OS of patients with a ≥30% or <30% increase in circulating hsa-miR-155-5p. PFS was calculated as the time from the date of randomization to the date of the first documented evidence of tumor progression, last tumor assessment or death in the absence of disease progression. OS was calculated as the time from the date of randomization to the date of death from any cause or last follow-up. Please click here to view a larger version of this figure.
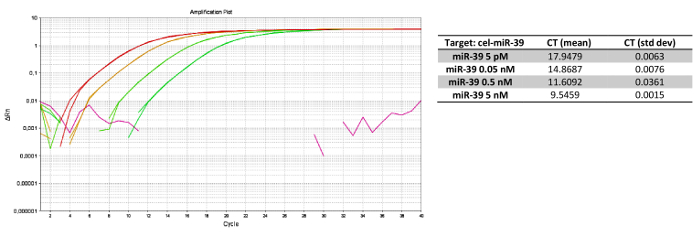
Figure 4: Experimental results forcel-miR-39 serial dilution. (A) qRT-PCR for serial dilutions of cel-miR-39, with (B) relative Cts. Dilutions were performed at 5 nM, 0.5 nM, 0.05 nM and 5 pM in plasma samples from the same patient. Such assay linearity enabled us to select the best concentration to use in the overall case series. Please click here to view a larger version of this figure.
| Step | Temperature | Duration | Cycles |
| Enzyme activation | 95 °C | 5 min | 1 |
| Denature | 95 °C | 3 s | 14 |
| Anneal/extend | 60 °C | 30 s | |
| Stop reaction | 99 °C | 10 min | 1 |
| Hold | 4 °C | Hold | ∞ |
Table 1: Thermal protocol of mir-AMP reaction.
| Step | Temperature | Duration | Cycles |
| Enzyme activation | 95 °C | 20 s | 1 |
| Denature | 95 °C | 3 s | 40 |
| Anneal/extend | 60 °C | 30 s | |
| Hold | 4 °C | Hold | ∞ |
Table 2: Thermal protocol of qRT-PCR.
