Surgeries were performed in approximately one hour by one surgeon with the help of one assistant. After surgical optimization, intra- and postoperative complications were greatly minimized and use of the jig apparatus ensured consistent size (5 x 3 x 3 mm) and localization of femoral defects. Rats were ambulatory immediately following recovery from anesthesia and did not appear to have any altered behavioral patterns; their gait was not antalgic, and they did not appear to be disturbed by the external fixator.
Non-threaded k-wires were chosen for the most proximal pin (Figure 2B), as the proximal pin had the highest risk of breaking when threaded wires were used. In some instances, particularly in control animals without rhBMP-2 or scaffolds whose defects showed no evidence of healing/bone formation, one or more k-wire tips broke after about 8 weeks as seen in the sponge only control radiograph of the excised femur (Figure 3).
Radiographs and histology (H&E stain) were analyzed to assess levels of bone healing. Negative control defects containing only a collagen sponge showed no evidence of bridging osteogenesis between the proximal and distal bone edges (Figure 3, Figure 4). A small amount of new bone remodeling can be seen directly adjacent to the cut femur edge; the defect itself shows a lack of bony material, the presence of cartilage, and some residual hematoma (Figure 4). Defects containing rhBMP-2 soaked sponge demonstrated significant bone healing as early as 4 weeks after surgery, as shown by the radiopaque callous bridging across the defect in Figure 3. By 12 weeks, significant new mineral deposition (Figure 4, NB: new bone, PC: periosteal callous) has formed throughout the defect. Significant new periosteal bone can be seen in the callous extending from the cut femur edge, and spicules of woven and lamellar bone have developed throughout the defect. Cartilage deposition is not seen (Figure 4).
Histology (H&E stain) was also performed for both an uninfected control and an example of an infected femur (Figure 5). The infected femur is significantly enlarged, showing signs of an endosteal reaction infiltrating the bone cortex. Arrows indicate areas of osteoclast-mediated pathologic bone resorption. The uninfected femur cortex remains compact and with a clearly delineated lamellar cortex. Antibiotic dosing was optimized to include maximal coverage postoperatively. While infection around the defect site can occur, continued administration of antibiotics topically around pin sites and in water and diet proved successful in minimizing postoperative infection.
Further imaging using In Vivo Imaging System (IVIS) illustrates the ability of bioluminescent cells to be visualized within the defect after implantation of the external fixator (Figure 6). The external plate can be easily removed for imaging and replaced upon completion. Cells in the medullary cavity luminesce after transfection with complexed mRNA encoding for Gaussia luciferase. The highest level of luminescence is focused at the site of the femoral defect and the signal is not obstructed by the fixation device pins. This is promising for future studies relying on bioluminescence or fluorescence to measure biological changes such as a gene or protein expression during the healing process.
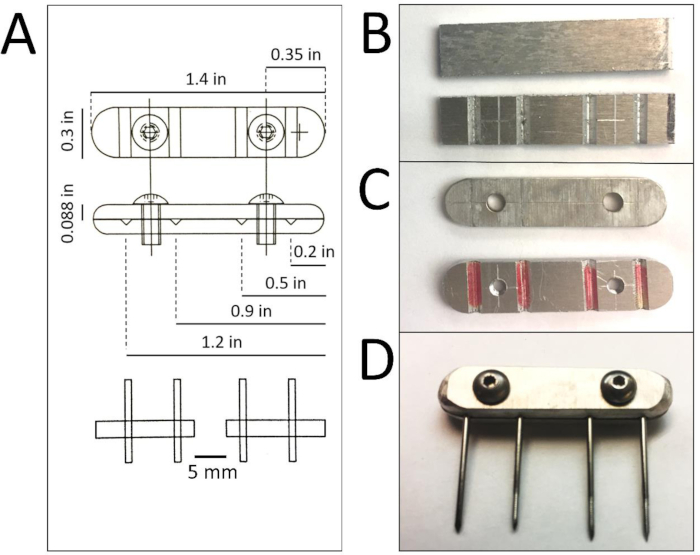
Figure 1: External fixator fabrication. A: CAD schematic of the assembled external fixator with annotated dimensions for proper fabrication. Each fixator is composed of two aluminum plates held together by two screws. B: Plates are cut from 1.4” x 6” aluminum sheets with ‘V’ grooves cut into the bottom sheet. C: Screw holes are drilled into the plates (threaded in the plate with ‘V’ grooves) and all edges and corners are sanded to round and reduce weight. D: Assembled external fixator is tightened with screws (4-40 x 0.25”, 18-8 stainless steel button head cap) once pins are in place in the ‘V’ grooves on the insides of the aluminum plates. The left pin is non-threaded and is most proximal on the femur. Please click here to view a larger version of this figure.
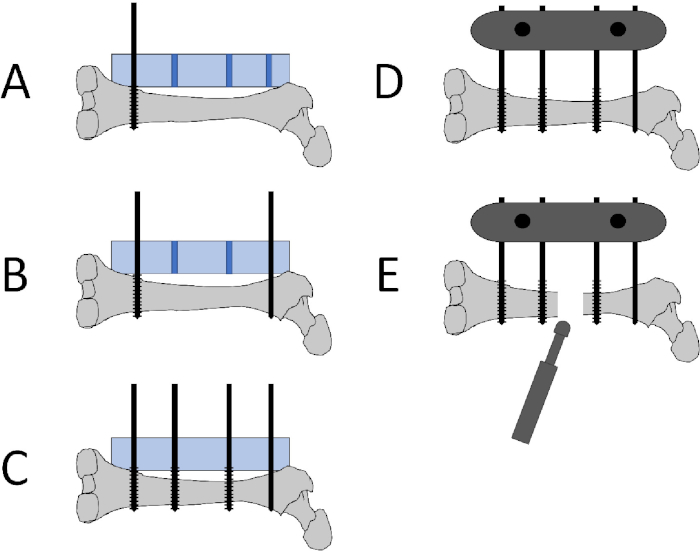
Figure 2: Schematic of pin placement, fixator placement, and defect creation. A: The distal pin (1.0 mm threaded k-wire) is placed at the epicondyle metaphyseal region using the jig (blue rectangle) to guide proper pin insertion. The jig is placed onto the anterolateral femoral surface. B: The proximal pin (1.0 mm non-threaded k-wire) is placed using the jig after making a small incision in the gluteal tendon. C: The middle pins (1.0 mm threaded k-wire) are inserted using the jig. D: The jig is removed and the 2 plates are attached to the pins using the 2 screws to secure the plates. The plates are tightened 1 cm above skin level to avoid pressure on the skin. E: A sagittal oscillating saw is used to create a 5 mm defect between the two middle pins. Please click here to view a larger version of this figure.
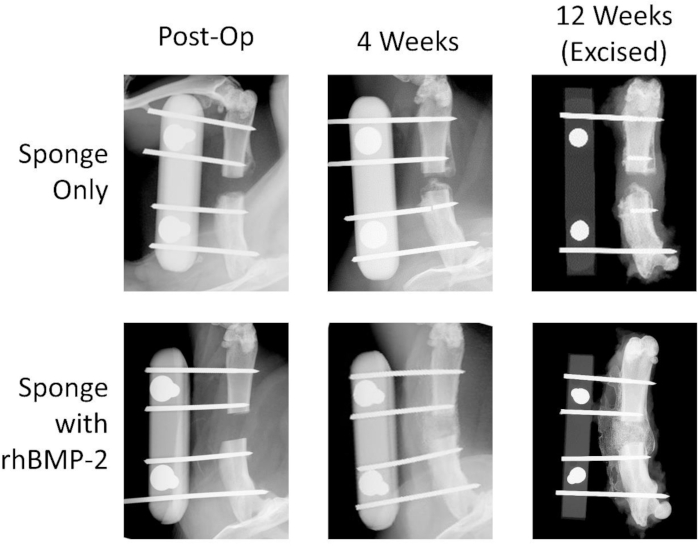
Figure 3: Representative high-resolution radiographs show bone healing with rhBMP-2 treatment. Images for the negative control collagen sponge and the rhBMP-2 soaked sponge groups are shown at 0, 4, and 12 weeks postoperatively. The rhBMP-2 treatment group exhibits significant healing after 4 weeks with callous spanning the defect. The negative control femur ends do not heal with bridging bone and the defect remains a non-union. Please click here to view a larger version of this figure.
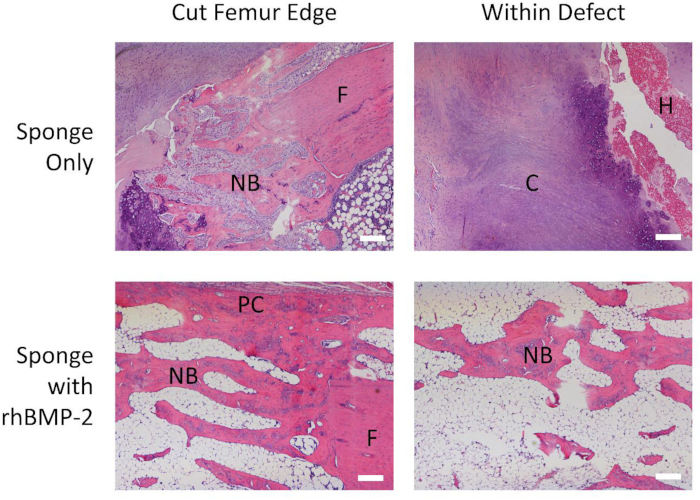
Figure 4: Significant new bone formation is seen with rhBMP-2 treatment. Representative 4x magnified H&E histological images for the negative control collagen sponge and the rhBMP-2 soaked sponge groups both at the cut femur edge and within the defect. New bone formed around the control femur edge, but significant extensions of both new trabecular bone as well as the periosteal callous project from the treated femur. No bony material is seen within the control defect, while significant bone formation can be observed throughout the rhBMP-2 treated defect. NB: new bone, F: femur, C: cartilage, H: hemorrhage, PC: periosteal callous. Scale bar: 200 µm. Please click here to view a larger version of this figure.
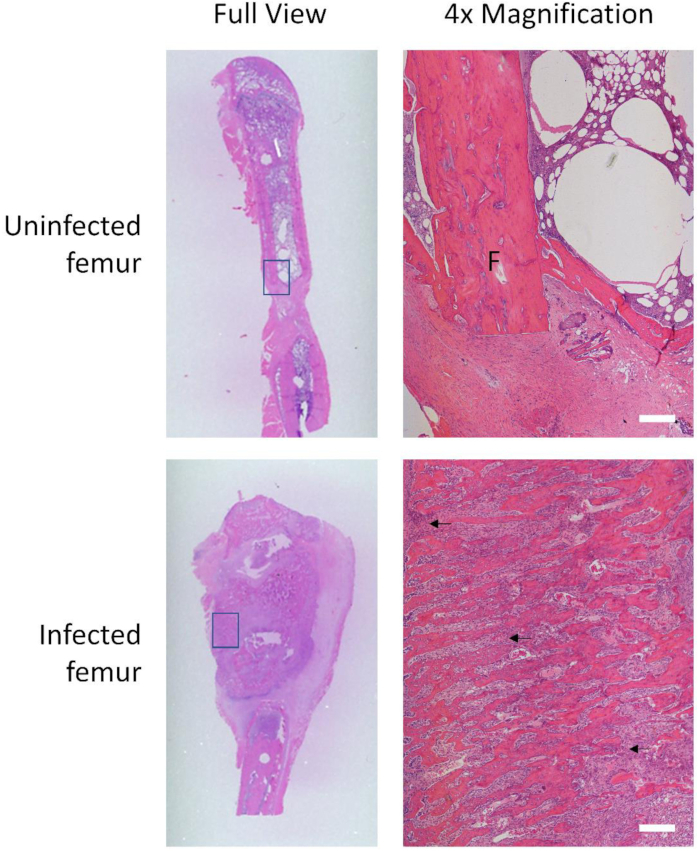
Figure 5: Infected femur exhibits hypertrophy and inflammatory cell markers. H&E histological images of an uninfected femur compared to an infected femur, in full view and at 4x magnification of boxed locations. The uninfected femoral cortex remains organized and delineated, with little sign of inflammation. The infected femur enlarges greatly, as seen in full view, and the cortex is broken up by areas of resorption and necrosis (purple cell clusters indicated by black arrows). F: femur. Scale bar: 200 µm. Please click here to view a larger version of this figure.
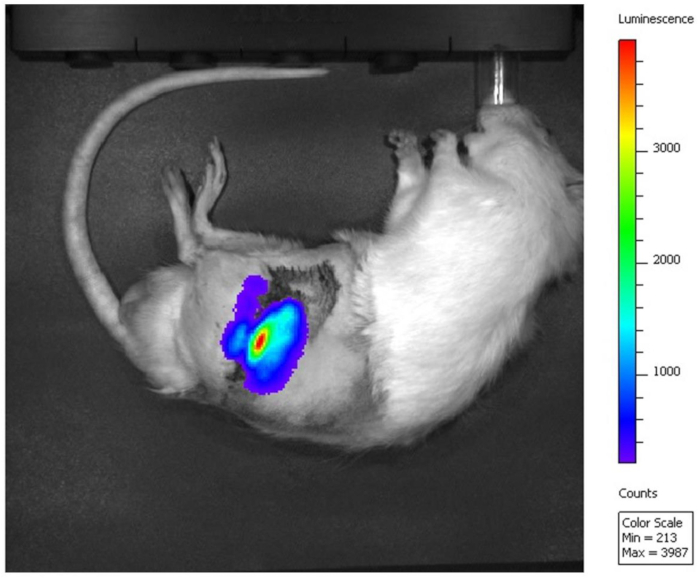
Figure 6: Gaussia luciferase signal detected in the defect. Luminescence of cells transfected with Gaussia luciferase mRNA is imaged with IVIS after external plate removal. Red indicates the highest luminescence intensity at the site of the femoral defect. Please click here to view a larger version of this figure.
