Calvarial Model of Bone Augmentation in Rabbit for Assessment of Bone Growth and Neovascularization in Bone Substitution Materials
Summary
Here we present a surgical protocol in rabbits with the aim to assess bone substitution materials in terms of bone regeneration capacities. By using PEEK cylinders fixed onto rabbit skulls, osteoconduction, osteoinduction, osteogenesis and vasculogenesis induced by the materials may be evaluated either on live or euthanized animals.
Abstract
The basic principle of the rabbit calvarial model is to grow new bone tissue vertically on top of the cortical part of the skull. This model allows assessment of bone substitution materials for oral and craniofacial bone regeneration in terms of bone growth and neovascularization support. Once animals are anesthetized and ventilated (endotracheal intubation), four cylinders made of polyether ether ketone (PEEK) are screwed onto the skull, on both sides of the median and coronal sutures. Five intramedullary holes are drilled within the bone area delimited by each cylinder, allowing influx of bone marrow cells. The material samples are placed into the cylinders which are then closed. Finally, the surgical site is sutured, and animals are awaken. Bone growth may be assessed on live animals by using microtomography. Once animals are euthanized, bone growth and neovascularization may be evaluated by using microtomography, immune-histology and immunofluorescence. As the evaluation of a material requires maximum standardization and calibration, the calvarial model appears ideal. Access is very easy, calibration and standardization are facilitated by the use of defined cylinders and four samples may be assessed simultaneously. Furthermore, live tomography may be used and ultimately a large decrease in animals to be euthanized may be anticipated.
Introduction
The calvarial model of bone augmentation was developed in the 90’s with the aim to optimize the concept of guided bone regeneration (GBR) in the oral and craniofacial surgical domain. The basic principle of this model is to grow new bone tissue vertically on top of the cortical part of the skull. To do so, a reactor (e.g., titanium -dome, -cylinder or -cage) is fixed onto the skull to protect the bone regeneration conducted by a graft (e.g., hydrogel, bone substitute, etc.). With the aid of this model, titanium or ceramic cages1,2,3,4,5,6, GBR membranes7,8,9,10, osteogenic factors11,12,13,14,15,16,17, new bone substitutes12,16,17,18,19,20,21,22,23,24,25,26,27,28,29 or the mechanism of neovascularization during the bone regeneration process30 were assessed.
From a translational point of view, the calvarial model represents a one-wall defect that can be compared to a class IV defect in the jaw31. The aim is to grow new bone above a cortical area, without any lateral support from endogenous bone walls. The model is thus extremely stringent and assesses the real potential of vertical osteoconduction over the cortical part of the bone. If the model described herein is primarily dedicated to the assessment of osteoconduction in bone substitutes, osteogenesis and/or osteoinduction may be also assessed, as well as vasculogenesis1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30.
Essentially for ethical, practical and economic reasons, the calvarial model was developed in the rabbit in which the bone metabolism and structure are quite relevant when compared to human32. Of the 30 references cited above, 80% used the rabbit calvarial model1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,17,22,23,26,27,28,29,30,33, thus demonstrating the relevance of this animal model. In 2008, the Busenlechner group transferred the calvarial model to the pig, to allow the comparison of eight bone substitutes simultaneously20 (as compared to two bone substitutes with the rabbit). On the other hand, our group transferred the rabbit calvarial model to sheep. In brief, titanium domes were placed on sheep skulls to characterize the osteoconduction of a new 3D-printed bone substitute. These studies allowed us to develop and master the calvarial model and its analysis16,21.
The last three studies cited16,20,21, together with several other investigations12,17,18,19,22,23,24,26,27,28,29, confirmed the great potential of the calvarial model as a screening and characterization model. However, even though the results obtained were quite satisfactory, they also pointed out some limitations: (1) The use of titanium domes, which prevented X-ray diffusion and in turn live micro-CT use. These could not be removed before histological processing, forcing the researchers to embed the samples in poly(methyl methacrylate) resin (PMMA). The resulting analyses were therefore largely limited to topography. (2) High financial costs especially because of the cost of the animals, and costs related to the logistics, maintenance and the surgery of the animals. (3) Difficulties to obtain ethical approvals for large animals.
A recent study by Polo, et al.26 largely improved the model on the rabbit. Titanium domes were replaced by closable cylinders that could be filled with a constant volume of material. Four of these cylinders were placed on rabbit skulls. At completion, the cylinders could be removed so that biopsies were metal-free, introducing much more flexibility concerning sample processing. The rabbit calvarial model became attractive for simultaneous testing with lower costs, easy animal handling and facilitation of sample processing. Taking advantage of these recent developments, we have further improved the model by replacing titanium with PEEK to produce cylinders, thereby allowing X-ray diffusion and the use of microtomography on live animals.
In this article, we will describe the anesthesia and surgery processes and show examples of outputs that may be obtained using this protocol, i.e., (immuno-) histology, histomorphometry, live and ex vivo microtomography to evaluate the mechanisms of bone regeneration and quantify the new bone synthesis supported by bone substitute materials.
Protocol
In line with Swiss legal requirements, the protocol was approved by an academic committee and supervised by the cantonal and federal veterinary agencies (authorizations n° GE/165/16 and GE/100/18).
1. Specific devices and animals
- Cylinders
- Machine cylinders with lateral stabilizing tabs out of PEEK to have inner diameter of 5 mm, outer diameter of 8 mm and a height of 5 mm (Figure 1).
- Machine PEEK caps with a design allowing to clip precisely onto the top of the cylinder (thickness 1 mm).
- Sterilize PEEK cylinders and caps by autoclaving before surgery.
- Screws
- Use self-drilling micro screws (made of commercial pure titanium (grade 5)) to fix the cylinders (1.2 mm in diameter, 4 mm in length). Sterilize by autoclaving before surgery.
- Animals
- Purchase three-month-old New Zealand white rabbits (male or female), weighing ~2.5 kg each.
NOTE: We obtained rabbits by breeding at the University of Geneva.
- Purchase three-month-old New Zealand white rabbits (male or female), weighing ~2.5 kg each.
2. Surgery
- Surgical tray
- Keep scalpels, scissors, two forceps, periosteal elevator, syringes (1, 2, 5, 50 mL), surgical motor, round surgical burs (0.8 mm diameter), needles, sterile saline, four cylinders, eight screws, and screwdriver ready.
- Preclinical treatment
- Acclimate the animals one week prior to surgery.
- Provide a prophylactic antibiotic daily (5–10 mg/kg by mouth (PO)) starting 2 h before surgery up to 3 days after surgery.
- Anesthesia and intubation
- Sedate the animals by intramuscular (IM) injection of ketamine (25 mg/kg, 50 mg/mL, 0.5 mL/kg) + xylazin (3 mg/kg, 20 mg/mL, 0.15 mL/kg). Wait ~20 min for the animals to sleep
deeply (complete muscular atony).
NOTE: This premedication will allow a simple, fast and painless intubation process. Deep analgesia and anesthesia is induced as described in step 2.3.8. - Place an intravenous (IV) cannula into the marginal vein from the ear and keep it closed until intubation is completed.
NOTE: This IV line will serve to perfuse fentanyl and propofol for deep analgesia and anesthesia, respectively (see step 2.3.8). - Maintain anesthesia by supplying 5% sevoflurane in pure oxygen until intubation is performed.
NOTE: This step is necessary only if the animal shows signs of awakening (eye movements, muscular contractions). - Anesthetize the trachea locally by spraying 10% lidocaine. Place the rabbit in prone position and maintain its head in vertical extension.
- Slide the first endotracheal tube of small diameter (2.5 mm) into the rabbit trachea until airflow can be heard in the tube. This will open the larynx and facilitate the insertion of the definitive tube.
- Insert a guide (intubation catheter) in the tube to fix the position of the tube into the trachea. Remove the small diameter tube and slide the definitive endotracheal tube (4.9 mm) on the guide.
- Remove the guide and inflate the balloon at the end of the endotracheal tube to seal and block the device into the trachea. The tube will stay in place but it may be secured by using a lace tied around the forehead. Immediately ventilate (7 mL/kg, frequency of 40/min) the animal with 3% sevoflurane in pure oxygen.
- Continuously perfuse (ear vein) fentanyl (0.01 mg/mL, 2–4 mL/h) to induce analgesia, 2–4 mg/kg of (2%) propofol (20 mg/mL, 4–8 mL/h) to induce anesthesia, and 4 mL/kg/h of Ringer's acetate to maintain iso-volumetric conditions.
- Place a rectal temperature probe. Also monitor heart function, temperature and oxygen saturation during the entire process.
- Control the depth of anesthesia by monitoring autonomous breathing; if the animal shows signs of autonomous breathing, dispense a small bolus of propofol and fentanyl.
- Sedate the animals by intramuscular (IM) injection of ketamine (25 mg/kg, 50 mg/mL, 0.5 mL/kg) + xylazin (3 mg/kg, 20 mg/mL, 0.15 mL/kg). Wait ~20 min for the animals to sleep
- Site preparation
- Place the rabbit on a heated pad (39 °C) covered by a mattress pad (to avoid burns) on the surgery table. Shave the scalp.
- Apply a lubricating gel on the eyes to avoid irritation and dryness. Disinfect the site by scrubbing the skin with povidone iodine (10%). Then drape the rabbit with a sterile surgical drape and cut out an access area for the skull.
- Disinfect the surgical site with povidone iodine (10%) for a second time. Apply a lubricating gel on the eyes to avoid irritation and dryness.
- Prepare a draped table (sterile drape) on which to place the complete surgical tray.
- Surgical site opening
- Anesthetize locally with a subcutaneous (SC) injection of lidocaine 2% (1 mL) on the skull.
- Incise through the skin (with a scalpel) along the calvarial sagittal line, from the orbits to the external occipital protuberance (~4 cm in length). Ensure that the periosteum is incised.
- Gently elevate the periosteum (with a periosteal elevator) on both side of the incision. Rinse the site with sterile saline.
- Cylinder placement
- Locate the median and coronal sutures on the skull (Figure 2A,B). Note that these anatomical lines form a cross. The cylinders will be placed in each of the quadrants defined by the cross, ensuring that the edge of the cylinder is not over the suture (Figure 2C).
- Place the first cylinder on the left upper quadrant (left frontal bone), and try to lay the device flat. Fix in the position with strong hand pressure and screw a micro-screw, until resistance is felt. Ensure that the screw head is flush with the surface of the cylinder tab.
- Repeat the same procedure on the other tab to fix the cylinder tightly onto the skull. Ensure that the cylinder is hermetically fixed to the bone.
- Repeat the procedure on the right upper quarter (right frontal bone), left lower quarter (left parietal bone) and right lower quarter (right parietal bone).
- Bone drilling of 5 intramedullary holes within the area circumscribed by the cylinders (Figure 1)
- Drill an intramedullary hole under saline irrigation (0.8 mm in diameter, ~1 mm in depth) with a round bur on the bone, in the center of the area circumscribed by the cylinder. Ensure that bleeding appears.
- Drill two more intramedullary holes along the axis passing through the two tab screws, at the inner edges of the cylinder. Along the perpendicular axe, drill two more intramedullary holes at the inner edges of the cylinder. Ensure that bleeding appears.
- Repeat the operation within the three other cylinders.
- Filling cylinders with material samples and capping (Figure 3)
- Prepare the desired bone substitute material according to manufacturer instructions or material specifications.
- Fill the first cylinder to the brim with the material sample and close the cylinder by fitting the cap. Repeat the process in the 3 other cylinders.
- Surgical site closure
- Close the skin above the cylinders with an intermittent non-resorbable suture.
- Apply a sprayable dressing onto the wound.
3. Post-surgical treatment
- Stop analgesia and anesthesia (propofol and fentanyl perfusion arrest) supply and check the recovery of autonomous breathing.
- Stop the ventilation once the animal has recovered autonomous breathing. Maintain the animal under pure oxygen before complete awakening.
- Inject buprenorphine hydrochloride SC (0.02 mg/kg, 0.03 mg/mL, 0.67 mL/kg) and repeat the injection every 6 h for 3 days as post-surgical analgesia.
- Transfer the animal into its usual housing with water and complete feeding.
- Remove the sutures after about 10 days of wound healing.
Representative Results
The model described herein is dedicated to the assessment of osteoconduction in bone substitutes. Osteogenesis and-or osteoinduction of bone substitutes either (pre-)cellularized or loaded with bioactive molecules may be also assessed, as well as vasculogenesis1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30. A kinetic study may be used, from 3 days up to 3 months after surgery depending on the mechanisms and outputs to be analyzed. A classical timeline allowing descriptions at early and mid-time is: 2, 4, 6, 8 and 12 weeks. Note that a minimum of 6 samples per time point is mandatory to obtain significant results. Each sample to be tested needs to be placed at least one time in each position onto the skull per time point (random allocation). Finally, sham samples (e.g., cylinders filled with coagulated blood) have to be included in the protocol34.
Once the surgery is completed, bone growth may be monitored at different time points by using bone tomography on live animals. An example is shown in Figure 4A,B. Additional analysis requires animals to be sacrificed (lethal intravenous injection of 150 mg/kg pentobarbital (100 mg/mL). After euthanasia, samples are sectioned and cylinders are carefully removed (Figure 5). Biopsies are fixed with a solution of phosphate-buffered saline and 4% formaldehyde. Bone growth may then be assessed by using microtomography (Figure 4 C,D). Samples may also be processed for (immune-) histological staining. Histomorphometric analysis and specific stainings are then possible to complete the analysis more specifically (Figure 6).
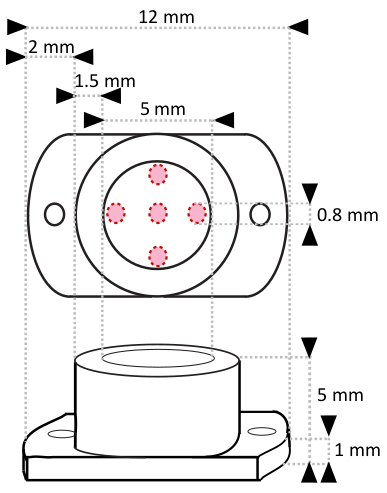
Figure 1: Specifications of PEEK cylinders. Two holes (0.8 mm in diameter) were drilled on the lateral stabilizing tabs for screwing. The positions of the 5 intramedullary holes (0.8 mm in diameter) to be drilled on the skull within the area delimited by the cylinder are marked using red circles. Please click here to view a larger version of this figure.
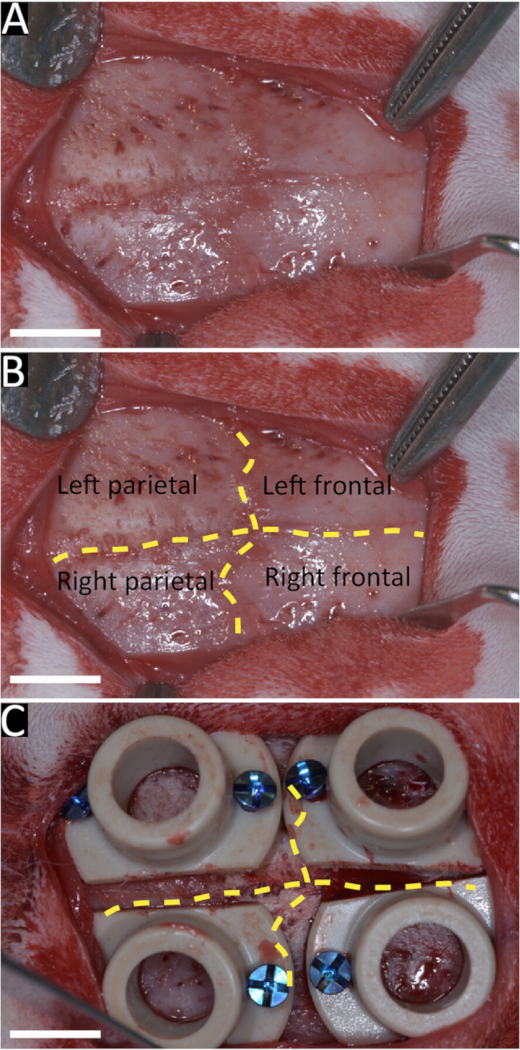
Figure 2: Representative image of the rabbit skull and placement of the cylinders. Pictures showing the median and coronal sutures on the rabbit skull delineating the left-right parietal and frontal bones (A,B). Placement of the cylinders on both side of the sutures (C). Scale bars = 5 mm. Please click here to view a larger version of this figure.
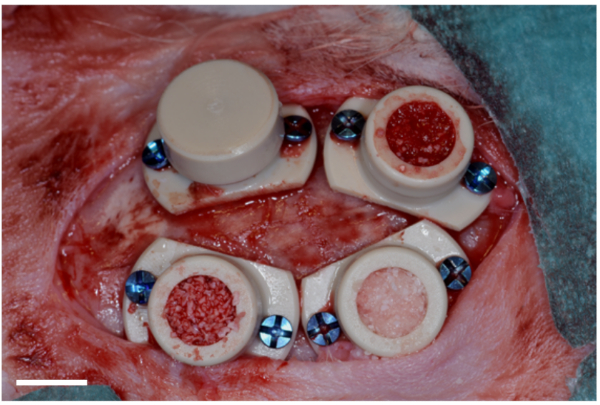
Figure 3: Representative image of cylinders fixed, filled and caped. Picture showing four cylinders fixed onto the skull of a rabbit with titanium screws. Within the area delimited by each cylinder, 5 intramedullary holes (0.8 mm in diameter, ~1 mm in depth) were drilled under irrigation with a round bur to allow bone cell migration. Cylinders were filled with different bone substitute samples (calibrated volumes) before capping (one closed cylinder is shown only). Scale bar = 5 mm. Please click here to view a larger version of this figure.
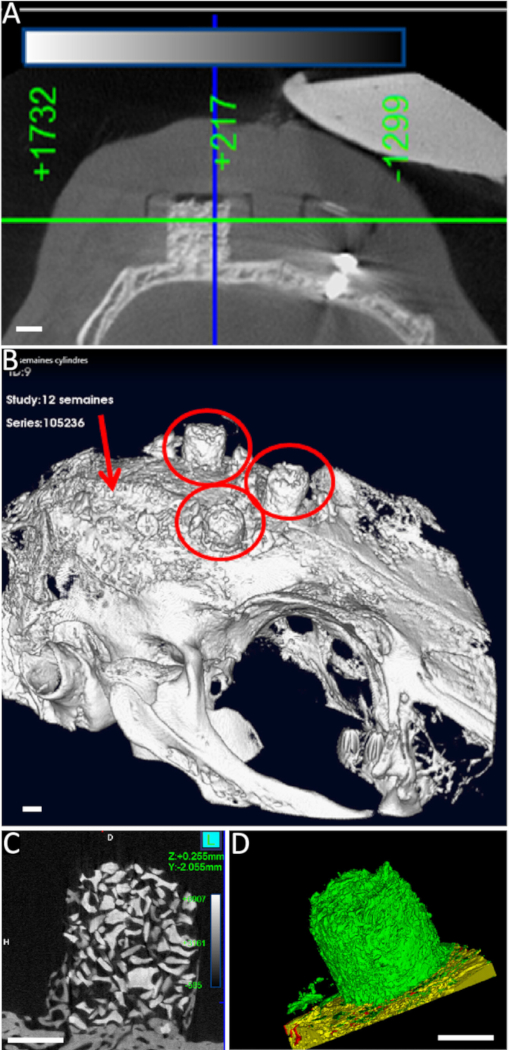
Figure 4: Representative images from microtomographic (micro-CT) analysis. With the final goal to assess bone growth conducted by bone substitutes, 4 cylinders were fixed onto a rabbit skull with titanium screws and filled with bone substitute materials. (A) Live imaging: two-dimensional transverse scan (14 min, 99 kV/88 µA with a resolution of 20 μm) of a cylinder at 12 weeks. (B) three-dimensional (3D) reconstruction from live micro-CT analysis at 4 weeks (red circles: bone substitutes in cylinders; red arrow: control in which the cylinder is filled with coagulated blood). (C,D) After euthanasia (12 weeks), cylinders were removed before fixation and micro-CT analysis. (C) 2D transverse scan (57 min, 99 kV/88 µA with a resolution of 10 μm) of a cylinder and 3D-reconstruction of the total new bone in the cylinder (D). Bone substitute particles (red), new bone (green) and bone bed (yellow) are shown. Scale bars = 2 mm Please click here to view a larger version of this figure.
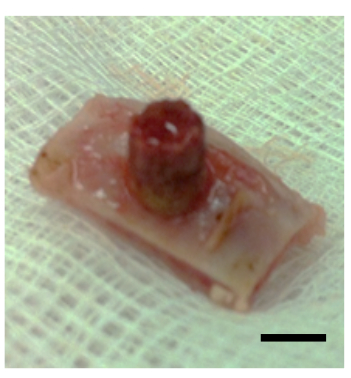
Figure 5: Representative images of a biopsy at 4 weeks. After euthanasia (4 weeks), samples were block-sectioned and cylinders were removed before fixation in 4% formalin, micro-CT analysis and histological processing. Scale bar = 5mm. Please click here to view a larger version of this figure.
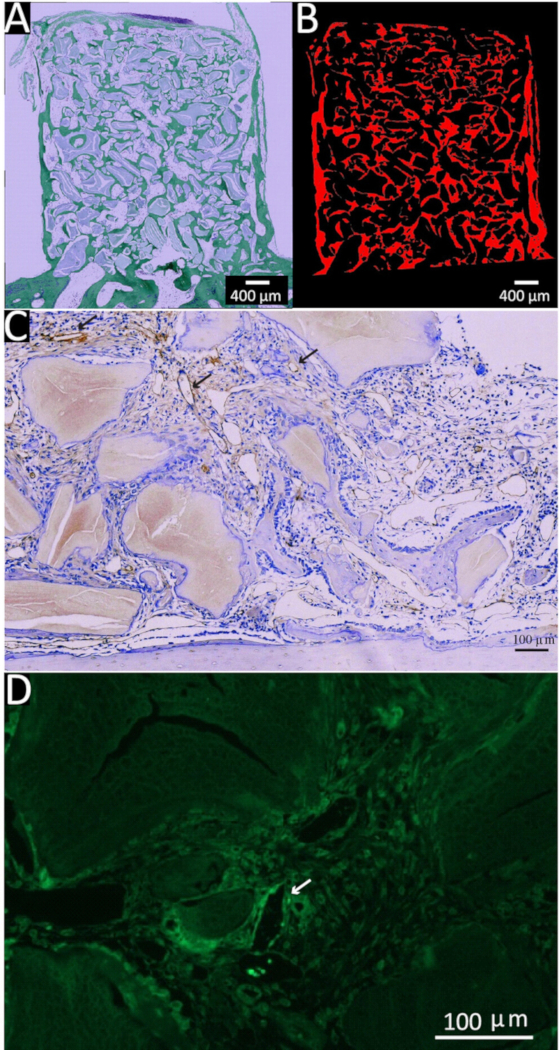
Figure 6: Representative pictures of (immune-)histological sections. With the final goal to assess bone growth and neovascularization conducted by bone substitutes, 4 cylinders were fixed onto a rabbit skull with titanium screws and filled with bone substitutes. After euthanasia (12 weeks), cylinders were removed before fixation and histological processing. (A) Masson-Goldner staining (50x): bone substitute appears as mauve particles surrounded by new bone in green. (B) The slices were scanned and processed for digital extraction of bone substitute material so that the new bone (red) could be quantified easily. (C) Immunostaining of CD31 (arrows), a typical marker of endothelial cells and the neovascularization process. (D) Immunofluorescent staining (green) of a highly neovascularized zone in which some new capillaries highly express CD31 (arrow). Please click here to view a larger version of this figure.
Discussion
The model described herein is simple and should be developed quite easily as long as all the steps are followed and the equipment is suitable. As the protocol described is a surgical method, all the steps appear critical and must be followed properly. It is critical to be trained for animal experiments, especially in rabbit handling and anesthesia. Do not hesitate to ask for professional anesthetist and veterinary help. It is critical to insist on the daily visual monitoring of animals before and after suture removal. Even if the skin from the skull is thick, abundant and loose, the cylinders’ fixation induces large tensions. If the sutures are removed too early, the wound might reopen and will require one more week of suturing and a new antibiotic treatment. In case of dehiscence out of the wound line, the surgeon will have to consider if suturing is possible or not. If not, sample rejection will have to be considered.
In addition to the critical steps described in the protocol section, the details below may be helpful in the proper implementation of this protocol. From a technical point of view, as the rabbits used are young and small, it is important to use a two-step intubation, as described in the protocol. The second (and final) tube is too large to be used in first intubation, and there is a real risk of “wrong way” that may be deleterious or even fatal.
Depending on the materials tested, it may be interesting to take some fresh blood sample from the ear IV line that is already placed. This could provide a good method to pre-infuse the bone substitute material with natural cells and growth factors. Freshly coagulated blood may also provide an ideal sham sample.
The way the intramedullary holes are drilled should be very helpful for future histological processing and histomorphometrical analysis. In effect, as long as the holes are (i) in the same location, (ii) the biopsies are similarly oriented and (iii) the cutting process is standardized (i.e., same thickness, same cut level), the fields that are evaluated are equivalent and their comparison is highly pertinent. As a matter of standardization, it may be of real interest to calibrate the volume-quantity of material to fill the cylinder, and to prepare it in advance, in a sterile way.
From a scientific point of view, depending on the products or hypothesis tested, it may be important to avoid placing the cylinders onto bone sutures. Some specific stem cells are present in these structures35, different from the mesenchymal bone stem cells that are involved in the mechanisms of intramembranous ossification, i.e., the bone regeneration process encountered in the orofacial area. Therefore, a real bias may occur in case of misplacement.
One of the major advantages of the calvarial model is the use of live microtomography by which the bone growth may be followed on a single animal as a longitudinal study. This strategy may largely reduce the number of euthanized animals and therefore respect the “3R rule”36. Depending on the microtomograph device used (resolution, space available for the animal), variations will occur in terms of strategy of anesthesia (IV, gas, etc.), as well as in the image resolution and the relevance of the resulting analysis.
We routinely use a microtomograph dedicated to animal experiments (e.g., Quantum GX) for routine checks. A typical experiment starts with a sedation, as described in step 2.3.1. Anesthesia is then maintained with 2% isoflurane in pure oxygen. This allows the animal to breathe calmly during a scanning time of about 14 min (99 kV/88 µA with a resolution of 20 μm); this is sufficient for checking basic parameters (engraftment, cylinder fixation, semiquantitative analysis of the bone growth, etc.). When looking for a precise qualitative and quantitative analysis, a very fine tuning of the scanning time, resolution, anesthesia and animal positioning will be needed.
Existing models developed for the assessement of osteoconduction, osteogenesis, osteoinduction as well as vasculogenesis, are numerous, especially in the orofacial field. Due to ethical and economic considerations, our purpose will be limited to rabbit or smaller animals. Apart from the skull, the locations in which the material may be tested are the mandibulla37,38,39,40,41,42,43,44,45,46,47, the diastema48 or the incisive sockets (after teeth extraction)49,50,51. Rats, mice, guinea pigs and rabbits may be used for each of the models described below. Briefly, a critical defect is drilled (or a socket is created by incisive extraction), filled with the material sample and then covered by a membrane. Apart from the obvious fact that only two samples can be tested in each of these locations (one sample per mandible side or per incisive socket), the surgical procedures are also largely more difficult and invasive. Accesses to the site are limited and if one is using rat or mice, the difficulty is further increased by the size of the animals. Finally, the critical size of the defects (i.e., dimensions that do not allow a spontaneous bone regeneration) is not well-defined and varies from one animal to another.
Besides these generalities, specific constraints may arise depending on the anatomical location subjected to the defect and to the subsequent analysis. As an example, in the mandibular model, teeth roots are present within the defect. This may interfere with the material and modify the bone regeneration process. The defect could be placed more distally on the ramus, but in that case, the bone would be very thin (two corticals affixed with an extremely thin medullary space) and the resulting defect volume may be too small45,46,47. Given these examples of limitations and depending on the model, large deviations may be anticipated in terms of material volume to be tested, quality and quantity of data collected.
As the evaluation of a material requires a maximum of standardization and calibration, the calvarial model appears ideal. Access is very easy, calibration and standardization are facilitated by the use of defined cylinders and 4 samples may be assessed simultaneously. Furthermore, live tomography may be used and finally a large decrease in animals to be euthanized may be anticipated.
Divulgations
The authors have nothing to disclose.
Acknowledgements
The authors are indebted to Geistlich AG (Wolhusen, CH) and the Osteology foundation (Lucerne, CH) (grant n°18-049) for their support, as well as Global D (Brignais, FR) for providing the screws. A particular thanks goes to Dr B. Schaefer from Geistlich. We are also grateful to Eliane Dubois and Claire Herrmann for their excellent histological processing and their precious advices. Finally, we warmly acknowledge Xavier Belin, Sylvie Roulet and the entire team of Pr Walid Habre, “experimental surgery Dpt” ,for their remarkable technical assistance.
Materials
| Drugs | |||
| Enrofloxacine Baytril 10% | Bayer | Antibiotic | |
| Fentanyl | Bischel | For analgesia | |
| Ketalar 50mg/ml | Pfizer | Ketamine for anesthesia | |
| Lidohex | Bichsel | Lubricating gel for the eyes | |
| Opsite | Smith and Nephew | 66004978 | Sprayable dressing |
| Povidone iodine 10%, Betadine | Mundipharma | anti-infective agent | |
| Propofol 2% | Braun | 3538710 | For anesthesia |
| Rapidocain 2% | sintetica | Local anesthesia | |
| Ringer-acetate | Fresenius Kabi | Volume compensation | |
| Rompun 2% | Bayer | Xylazin for anesthesia | |
| Sevoflurane 5% | Abbvie | For anesthesia | |
| Sterile saline | Sintetica | ||
| Temgesic | Reckitt Benckiser | Buprenorphine hydrochloride, analgesia | |
| Thiopental Inresa | Ospediala | For anesthesia | |
| Xylocaine 10% spray | Astra Zeneca | For intubation | |
| Name | Company | Catalog Number | Comments |
| Equipment | |||
| Fresenius Vial pilot C | Imexmed | Infusion pump | |
| Heated pad | Harvard Apparatus | ||
| Suction dominant 50 | Medela | ||
| Suction tubing Optimus | Promedical | 80342.2 | |
| Surgical motor | Schick dental | Qube | Drilling of intramedullary holes |
| Ventilation | Maquet Servo1 | ||
| Name | Company | Catalog Number | Comments |
| Material | |||
| Cylinders and caps | Boutyplast | Customized | composition: PEEK (poly ether ether ketone) |
| Manual self-retaining shaft | GlobalD | ACT1K | |
| Mobile handle for self-retaining shaft | GlobalD | MTM | |
| Self- drilling screws | GlobalD | VA1.2KL4 | cross-drive screws composed by Titanium grade5, ISO 5832-3 |
| Name | Company | Catalog Number | Comments |
| Surgical tray | |||
| Endotracheal tube Shiley diameter 2,5mm | Covidien | 86233 | For intubation |
| Endotracheal tube Shiley diameter 4,9mm | Covidien | 107-35G | For intubation |
| Ethicon prolene 4-0 | Ehticon | 8581H | Non-resorbable suture |
| Forceps | Marcel Blanc | BD027R | 145 mm |
| Intubation catheter | Cook medical | Guide for intubation | |
| Needlle holder | Marcel Blanc | BM008R | |
| Needles BD Microlance3 | Becton Dickinson | 300300/304622 | 26G; 18G |
| Periosteal | HU-Friedy | P9X | |
| Round surgical burs | Patterson | 78000 | 0.8 mm in diameter, Drilling of intramedullary holes |
| Scalpel | Swann-Morton | n°10 and n°15 | |
| Scissors | Marcel Blanc | 00657 | 180 mm |
| Syringes Omnifix | Braun | 4616057V | 5ml, 10ml and 50ml |
| Venflon G22 | Braun | 42690985-01 | Vasofix safety for the ear iv line |
References
- Anderud, J., et al. Guided bone augmentation using a ceramic space-maintaining device. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. 118 (5), 532-538 (2014).
- Lundgren, A. K., Lundgren, D., Hammerle, C. H., Nyman, S., Sennerby, L. Influence of decortication of the donor bone on guided bone augmentation. An experimental study in the rabbit skull bone. Clinical Oral Implants Research. 11 (2), 99-106 (2000).
- Lundgren, D., Lundgren, A. K., Sennerby, L., Nyman, S. Augmentation of intramembraneous bone beyond the skeletal envelope using an occlusive titanium barrier. An experimental study in the rabbit. Clinical Oral Implants Research. 6 (2), 67-72 (1995).
- Slotte, C., Lundgren, D. Impact of cortical perforations of contiguous donor bone in a guided bone augmentation procedure: an experimental study in the rabbit skull. Clinical Implant Dentistry and Relat Research. 4 (1), 1-10 (2002).
- Tamura, T., et al. Three-dimensional evaluation for augmented bone using guided bone regeneration. Journal of Periodontal Research. 40 (3), 269-276 (2005).
- Yamada, Y., et al. Correlation in the densities of augmented and existing bone in guided bone augmentation. Clinical Oral Implants Research. 23 (7), 837-845 (2012).
- Chierico, A., et al. Electrically charged GTAM membranes stimulate osteogenesis in rabbit calvarial defects. Clinical Oral Implants Research. 10 (5), 415-424 (1999).
- Ikeno, M., Hibi, H., Kinoshita, K., Hattori, H., Ueda, M. Effects of the permeability of shields with autologous bone grafts on bone augmentation. International Journal of Oral and Maxillofacial Implants. 28 (6), e386-e392 (2013).
- Ito, K., Nanba, K., Murai, S. Effects of bioabsorbable and non-resorbable barrier membranes on bone augmentation in rabbit calvaria. Journal of Periodontology. 69 (11), 1229-1237 (1998).
- Lee, Y. M., et al. Enhanced bone augmentation by controlled release of recombinant human bone morphogenetic protein-2 from bioabsorbable membranes. Journal of Periodontology. 74 (6), 865-872 (2003).
- Fugl, A., et al. S-nitroso albumin enhances bone formation in a rabbit calvaria model. International Journal of Oral and Maxillofacial Surgery. 43 (3), 381-386 (2014).
- Ikeno, M., Hibi, H., Kinoshita, K., Hattori, H., Ueda, M. Effects of self-assembling peptide hydrogel scaffold on bone regeneration with recombinant human bone morphogenetic protein-2. International Journal of Oral and Maxillofacial Implants. 28 (5), e283-e289 (2013).
- Ito, K., et al. Effects of ipriflavone on augmented bone using a guided bone regeneration procedure. Clinical Oral Implants Research. 18 (1), 60-68 (2007).
- Jung, R. E., Hammerle, C. H., Kokovic, V., Weber, F. E. Bone regeneration using a synthetic matrix containing a parathyroid hormone peptide combined with a grafting material. International Journal of Oral and Maxillofacial Implants. 22 (2), 258-266 (2007).
- Minegishi, T., et al. Effects of ipriflavone on bone augmentation within a titanium cap in rabbit calvaria. Journal of Oral Science. 44 (1), 7-11 (2002).
- Moussa, M., et al. Medium-Term Function of a 3D Printed TCP/HA Structure as a New Osteoconductive Scaffold for Vertical Bone Augmentation: A Simulation by BMP-2 Activation. Materials. 8 (5), 2174-2190 (2015).
- Thoma, D. S., Kruse, A., Ghayor, C., Jung, R. E., Weber, F. E. Bone augmentation using a synthetic hydroxyapatite/silica oxide-based and a xenogenic hydroxyapatite-based bone substitute materials with and without recombinant human bone morphogenetic protein-2. Clinical Oral Implants Research. 26 (5), 592-598 (2014).
- Busenlechner, D., et al. Resorption of deproteinized bovine bone mineral in a porcine calvaria augmentation model. Clinical Oral Implants Research. 23 (1), 95-99 (2012).
- Busenlechner, D., et al. Paste-like inorganic bone matrix: preclinical testing of a prototype preparation in the porcine calvaria. Clinical Oral Implants Research. 20 (10), 1099-1104 (2009).
- Busenlechner, D., et al. Simultaneous in vivo comparison of bone substitutes in a guided bone regeneration model. Biomaterials. 29 (22), 3195-3200 (2008).
- Carrel, J. P., et al. A 3D printed TCP/HA structure as a new osteoconductive scaffold for vertical bone augmentation. Clinical Oral Implants Research. 27 (1), 55-62 (2016).
- Murai, M., et al. Effects of different sizes of beta-tricalcium phosphate particles on bone augmentation within a titanium cap in rabbit calvarium. Dental Materials Journal. 25 (1), 87-96 (2006).
- Nishida, T., et al. Effects of bioactive glass on bone augmentation within a titanium cap in rabbit parietal bone. Journal of Periodontology. 77 (6), 983-989 (2006).
- Nyan, M., et al. Feasibility of alpha tricalcium phosphate for vertical bone augmentation. Journal of Investigating and Clinical Dentistry. 5 (2), 109-116 (2012).
- Polimeni, G., et al. Histopathological observations of a polylactic acid-based device intended for guided bone/tissue regeneration. Clinical Implant Dentistry and Related Research. 10 (2), 99-105 (2008).
- Polo, C. I., et al. Effect of recombinant human bone morphogenetic protein 2 associated with a variety of bone substitutes on vertical guided bone regeneration in rabbit calvarium. Journal of Periodontology. 84 (3), 360-370 (2013).
- Slotte, C., Lundgren, D., Burgos, P. M. Placement of autogeneic bone chips or bovine bone mineral in guided bone augmentation: a rabbit skull study. International Journal of Oral and Maxillofacial Implants. 18 (6), 795-806 (2003).
- Tamimi, F. M., et al. Bone augmentation in rabbit calvariae: comparative study between Bio-Oss and a novel beta-TCP/DCPD granulate. Journal of Clinical Periodontology. 33 (12), 922-928 (2006).
- Torres, J., et al. Effect of solely applied platelet-rich plasma on osseous regeneration compared to Bio-Oss: a morphometric and densitometric study on rabbit calvaria. Clinical Implant Dentistry and Related Research. 10 (2), 106-112 (2008).
- Yamada, Y., et al. Angiogenesis in newly augmented bone observed in rabbit calvarium using a titanium cap. Clinical Oral Implants Research. 19 (10), 1003-1009 (2008).
- Cordaro, L., Terheyden, H., Wismeijer, D., Chen, S., Buser, D. . ITI Treatment Guide. 7, (2014).
- Pearce, A. I., Richards, R. G., Milz, S., Schneider, E., Pearce, S. G. Animal models for implant biomaterial research in bone: A review. European Cells & Materials. 13, 1-10 (2007).
- Min, S., et al. Effects of marrow penetration on bone augmentation within a titanium cap in rabbit calvarium. Journal of Periodontology. 78 (10), 1978-1984 (2007).
- Braun, T. M., Giannobile, W. V., Nevins, M. Ch. 4. Osteology guidelines for oral and maxillofacial regeneration Preclinical models for translational research. , 31-43 (2011).
- Doro, D. H., Grigoriadis, A. E., Liu, K. J. Calvarial Suture-Derived Stem Cells and Their Contribution to Cranial Bone Repair. Frontiers in Physiology. 8, 956 (2017).
- Russel, W., Burch, R. . The principles of humane experimental technique. , (1959).
- Asvanund, P., Chunhabundit, P. Alveolar bone regeneration by implantation of nacre and B-tricalcium phosphate in guinea pig. Implant Dentistry. 21 (3), 248-253 (2012).
- Gielkens, P. F., et al. Gore-Tex as barrier membranes in rat mandibular defects: an evaluation by microradiography and micro-CT. Clinical Oral Implants Research. 19 (5), 516-521 (2008).
- Lioubavina, N., Kostopoulos, L., Wenzel, A., Karring, T. Long-term stability of jaw bone tuberosities formed by "guided tissue regeneration". Clinical Oral Implants Research. 10 (6), 477-486 (1999).
- Mardas, N., Kostopoulos, L., Stavropoulos, A., Karring, T. Osteogenesis by guided tissue regeneration and demineralized bone matrix. Journal of Clinical Periodontology. 30 (3), 176-183 (2003).
- Stavropoulos, A., Kostopoulos, L., Mardas, N., Nyengaard, J. R., Karring, T. Deproteinized bovine bone used as an adjunct to guided bone augmentation: an experimental study in the rat. Clinical Implant Dentistry and Related Research. 3 (3), 156-165 (2001).
- Stavropoulos, A., Kostopoulos, L., Nyengaard, J. R., Karring, T. Deproteinized bovine bone (Bio-Oss) and bioactive glass (Biogran) arrest bone formation when used as an adjunct to guided tissue regeneration (GTR): an experimental study in the rat. Journal of Clinical Periodontology. 30 (7), 636-643 (2003).
- Stavropoulos, A., Kostopoulos, L., Nyengaard, J. R., Karring, T. Fate of bone formed by guided tissue regeneration with or without grafting of Bio-Oss or Biogran. An experimental study in the rat. Journal of Clinical Periodontology. 31 (1), 30-39 (2004).
- Stavropoulos, A., Nyengaard, J. R., Kostopoulos, L., Karring, T. Implant placement in bone formed beyond the skeletal envelope by means of guided tissue regeneration: an experimental study in the rat. Journal of Clinical Periodontology. 32 (10), 1108-1115 (2005).
- Thomaidis, V., et al. Comparative study of 5 different membranes for guided bone regeneration of rabbit mandibular defects beyond critical size. Medical Science Monitor. 14 (4), (2008).
- Zhang, J. C., et al. The repair of critical-size defects with porous hydroxyapatite/polyamide nanocomposite: an experimental study in rabbit mandibles. International Journal of Oral and Maxillofacial Surgery. 39 (5), 469-477 (2010).
- Zhang, X., et al. Osteoconductive effectiveness of bone graft derived from antler cancellous bone: an experimental study in the rabbit mandible defect model. International Journal of Oral and Maxillofacial Surgery. 41 (11), 1330-1337 (2012).
- Bronoosh, P., et al. Effects of low-intensity pulsed ultrasound on healing of mandibular bone defects: an experimental study in rabbits. International Journal of Oral and Maxillofacial Surgery. 44 (2), 277-284 (2015).
- Gomes, F. V., et al. Low-level laser therapy improves peri-implant bone formation: resonance frequency, electron microscopy, and stereology findings in a rabbit model. International Journal of Oral and Maxillofacial Surgery. 44 (2), 245-251 (2014).
- Lalani, Z., et al. Spatial and temporal localization of secretory IgA in healing tooth extraction sockets in a rabbit model. Journal of Oral and Maxillofacial Surgery. 62 (4), 466-472 (2004).
- Osorio, L. B., et al. Post-extraction evaluation of sockets with one plate loss–a microtomographic and histological study. Clinical Oral Implants Research. 27 (1), 31-38 (2014).
