A microanalysis of video material (122 videos) collected for a qualitative, grounded-theory-based, multiperspective study of CMT23,50, identified three central interaction categories: 1) responsiveness of the therapist and parents, 2) resulting in communicative musicality with the infant, and 3) infants' and parents' empowerment as a consequence of categories 1 and 2 (Figure 1). The study results suggest that the therapists' prevailing attitude of responsiveness via musical attunement and entrainment may facilitate shared communicative musicality (e.g., interactional synchrony, moment of meeting, interplay). By experiencing this relatedness in music, parents and infants may be supported to relax and to engage in mutual relationship. However, preterm infants still act and re-act with most subtle facial expressions and movements23.
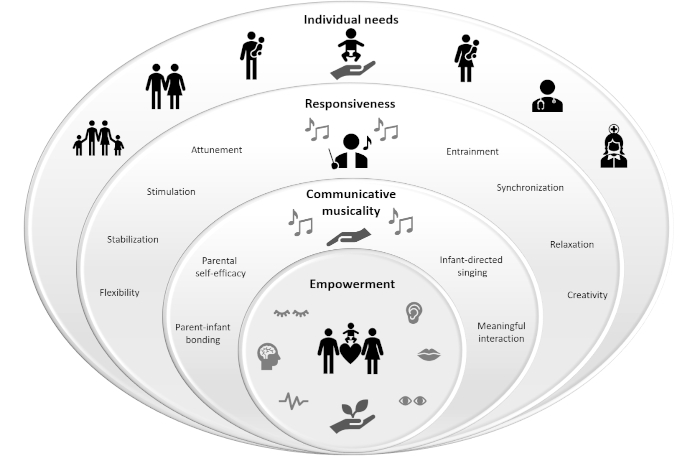
Figure 1: Logic diagram of categories inherent in the CMT process. This figure has been modified from Haslbeck23. Please click here to view a larger version of this figure.
In this context, responsiveness means the therapist`s ability to observe, interpret, and respond reasonably with musical capacity57. The video microanalysis revealed that when the infant is aroused, the therapist sings as simple and repetitive as possible to calm down the infant. The therapist softly hums only two long holding notes centering around the tonic of the scale to provide a musical holding, stability, and safety (Figure 2, blue circle voice line, 0:21-0:55). The therapist continually entrains the singing to the breathing rhythms of the infant (Figure 2-4: infant`s breathing and therapist`s voice line continuously rhythmically entrained).
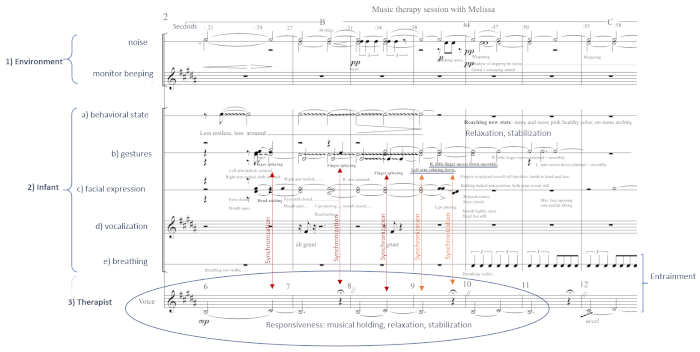
Figure 2: Transcription of responsiveness and therapist-infant synchronization. Detailed transcription of music therapy session with Melissa by using conservative music notation with Finale 2011 notation software50 including three layers on the same timescale: 1) environment, 2) infant behavior (four layers: a) behavioral state b) gestures c) mimicry d) breathing pattern, if visible) and 3) therapist`s voice. This figure has been modified from Haslbeck50. Please click here to view a larger version of this figure.
Further responsiveness involves attuning to the environmental sounds such as the monitor beeping. The therapist sings in the key of the monitor alarms (Figure 3, blue arrows, 1:00-1:07) to integrate sudden stressful digital sounds in the music and thereby to mitigate disturbing noises. Consequently, "Melissa" remains calm (Figure 3, blue rectangles, 1:04-1:10) after the sudden alarm during music therapy (Figure 3, red star, 1:04) in contrast to beeping noise evoked stressed reactions without music therapy50. The therapist continuously tailors the singing to the facial expressions and gestures of the infant (Figure 3, orange arrows, 0:58, 1:09). For instance, when Melissa smiles and rises her fingers the therapist rises the melody, tempo and dynamics synchronously (Figure 4, blue circle: compare voice line with breathing, mimic mouth and gesture line, 1:30-1:45).
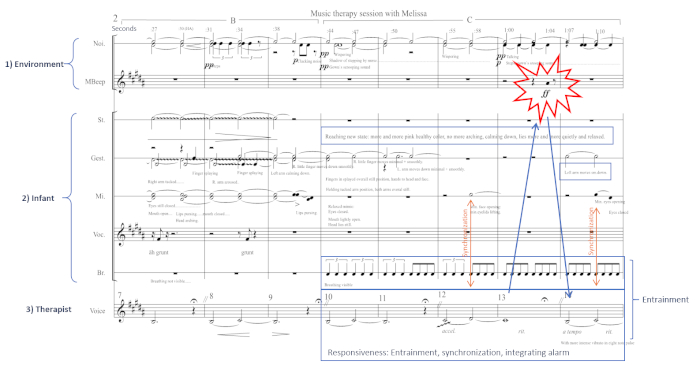
Figure 3: Transcription of responsiveness, entrainment, therapist-infant synchronization, and integrating of monitor alarm. Detailed transcription of music therapy session with Melissa as described in Figure legend 2. This figure has been modified from Haslbeck50. Please click here to view a larger version of this figure.
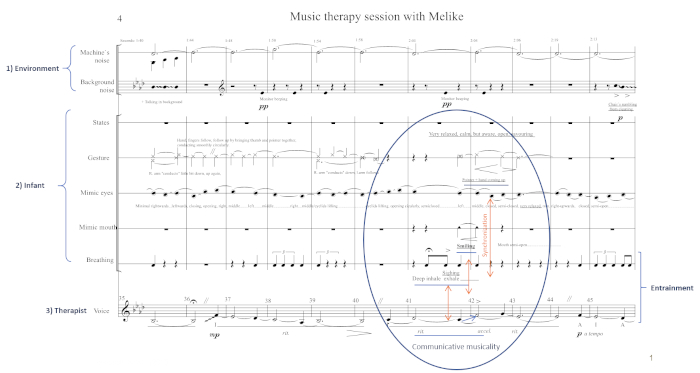
Figure 4: Transcription of communicative musicality and therapist-infant synchronization. Detailed transcription of music therapy session with Melissa as described in Figure legend 2. This figure has been modified from Haslbeck50. Please click here to view a larger version of this figure.
Communicative musicality acts like the intuitive affect attunement of a healthy caregiver-infant relationship. This sharing of emotional experiences is like a dance, like a musical performance52,58,59,60. Through shared rhythms, tempi, and affects, communicative musicality may support the infants' coregulation and stabilization and may transform the arrhythmic intensive care environment into a relational environment required for healthy socio-emotional development and growth59. The video microanalysis50 implies that CMT may enhance relaxation, participation, self-regulation, and engagement in premature infants through experienced communicative musicality. Communicative musicality can evolve through interactional synchronization of affects. In Figure 2, at first, Melissa synchronizes her stressed movements with the tension in the music. She splays her fingers synchronously with the higher more suspenseful note or in the tense pause (Figure 2, red arrows, 0:24-0:37). After synchronizing with the tension in the music, she may then be able to synchronize with the relaxation of the music. When the first musical phrase ends, she relaxes her body and moves her arms and fingers smoothly down (Figure 2, orange lines, 0:38-0:44). Throughout the session, Melissa remains in this relaxed behavioral state and engages with increasing smooth facial reactions and finger movements (Figure 3, orange arrows, 0:58 -1:09). When the melody rests with the ritardando (rit.), she sighs deeply (Figure 4, blue circle, orange arrow, 2:03) interpreted as a sign of relaxation. When the melody, dynamics, and intensity ascend, she raises her finger and smiles (Figure 4, blue circle, orange arrows, 2:03-2:05) interpreted as engagement in communicative musicality.
By relaxing and engaging the parents in meaningful, sensitive interactions with the infant, the parents may experience self-confidence, self-efficacy, and autonomy. They may thereby be empowered in their role as primary caregivers and participants. In this context, empowerment means to facilitate self-regulation in the infant and to uncover intuitive parental capacities for parental responsiveness that are often overshadowed by anxiety and stress23,47. Parents reported in the qualitative interviews of the study that they could relax and relate more intense to their infant through music therapy: "I notice when I can relax that I am much more connected, much more intense, much more closely connected with my daughter because of the music, because of the singing."23
The video microanalysis revealed that mothers who were stressed and distanced connected with their infants through meaningful vocal interaction. Figure 5 & Figure 6 show the microanalysis of shared mother-infant rhythms of a previously stressed and detached mother. The mother entrains her singing to the sucking rhythms of her daughter. She sings with "motherese" (infant-directed, with a loving tone and free voice, responsive with facial expression and gestures) rocking the infant in the rhythm of the song. "Emila" begins with her sucking pattern precisely at the beginning of the musical phrase of her mother (Figure 5 & Figure 6, orange arrows) except in bar 9 (Figure 5, red circle, 0:26). The mother immediately recognizes, interprets correctly, reacts appropriately and promptly with sensitivity as referred to as appropriate bonding behavior23. She reduces and ceases her singing to hold and readjust (Figure 5 & Figure 6, blue circle, 0:26-0:28). After this moment of readjustment, she begins the musical phrase again in synchrony with the sucking pattern of Emila (Figure 6, blue circle, 0:28 following). Mother and daughter meet once more within communicative musicality in shared pulse and quality. They connect in a mutual gaze at the end of the musical phrase, and the mother smiles (Figure 5, 0:28 following). Mother and daughter meet in a "neonatal moment of meeting" described as tender moments after birth to generate the attachment bond and the mother's self-confidence in her role as primary caregiver23. Immediately after this singing episode, the mother expressed her love and empowerment by picturing herself as a lion mother. She phrases her self-confidence and autonomy by the sentences' causal dependence (underlined): "If I would not have so much love, right? Then my daughter would have no chance to survive. I am like a lion."23
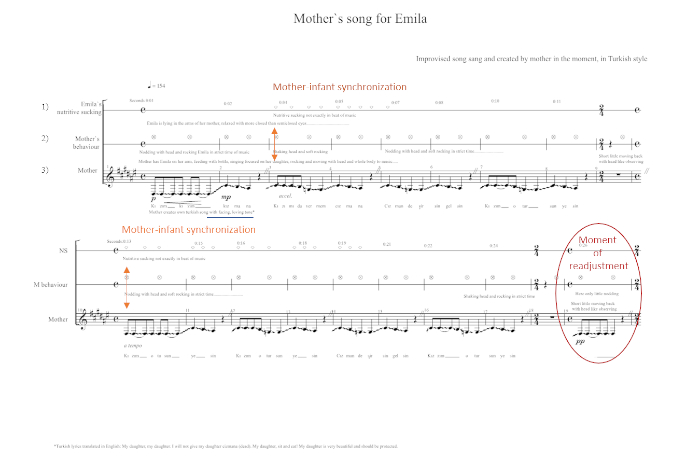
Figure 5: Mother-infant synchronization. Detailed transcription of mother`s singing for her daughter Emila by using conservative music notation with Finale 2011 notation software50 including three layers on the same timescale: 1) Emila`s nutritive sucking pattern, 2) mother`s behavior and 3) mother`s singing. This figure has been modified from Haslbeck23. Please click here to view a larger version of this figure.
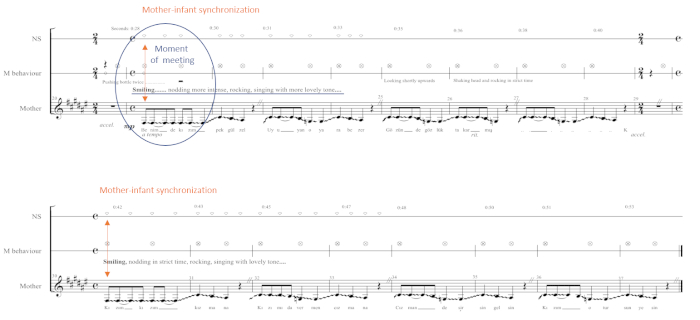
Figure 6: Mother-infant synchronization and moment of meeting. Detailed transcription of mother`s singing for her daughter Emila as described in Figure legend 5. This figure has been modified from Haslbeck23. Please click here to view a larger version of this figure.
First results of a mixed-method pilot trial underline these results. The study revealed that parental depressive symptoms decreased and physical closeness increased across hospitalization time in the CMT group compared to the control group27. The parents reported that CMT evoked feelings of relaxation and joy and empowerment to interact more profoundly with their infant27.
