All procedures were approved in accordance with the National Institutes of Health, the Guide for the Care and Use of Animals and were approved by both the Institutional Animal Care and Use Committee (IACUC) and Environmental Health and Safety at the University of Washington.
1. Calculation of angled coordinates
- Using a coronal brain atlas, mark a right triangle so that the hypotenuse passes through the target region of interest. In the representative example (Figure 1), the hypothalamic ventromedial nucleus (VMN) is targeted at a 15° angle from the coronal midline.
NOTE: The placement of the axis of rotation depicted in Figure 1 (and thus, the length of side C) is arbitrary and can be modified to target any brain region. Although this may seem counterintuitive, later steps in the protocol will adjust the position of the head in the z-axis such that this point aligns with the stereotactic center of rotation (see section 6). However, it is recommended not to exceed a coronal rotation angle of 15° due to physical constraints of the head holder apparatus. - Establish the desired angle (a) and estimated length of side B and use trigonometry to calculate the length of sides A and C. This step is important for properly positioning the head during rotation.
NOTE: In the example in Figure 1, atlas gridlines are used to approximate the length of side B, yielding a length of 7.576 mm. This information is used to calculate the length of side A:
In this example, 2.03 mm indicates the R/L distance from the midline at which the fiberoptic cannula enters the brain when the head is rotated by 15°.- Optionally, calculate the length of side C to approximate the D/V coordinate:

NOTE: 1) The length of the hypotenuse (C) does not represent the depth of injection but will be helpful in determining the D/V coordinate, which may need to be adjusted to accommodate for the increased length vs. side B for straight-in injections. It is therefore recommended to perform test injections to optimize the D/V coordinate. 2) In this example targeting the VMN, two sets of coordinates are obtained: one for the microinjection that is non-angled (A/P = -1.4, R/L = 0.4 at 0°, D/V = -5.7) and one for the angled fiberoptic implantation (A/P = -1.4, R/L = 0.0 at 15°, D/V = -5.4).
- Optionally, calculate the length of side C to approximate the D/V coordinate:
2. Preparation of the stereotax for angled procedure
- Confirm that the stereotactic frame and micromanipulator have been calibrated (see Kopf manual for full protocol).
- Place the center height gauge into the socket of the head holder base plate.
- Secure the centering scope in the tool holder, then sight down the scope. Adjust the position of the micromanipulator until the crosshairs are aligned and focused on the gauge crosshairs.
NOTE: During this step, the scope is being positioned into the focal plane of the head holder’s center of rotation. Once established, the micromanipulator should not be moved during the remaining steps. - Place the ear bars into the holders and center them such that the indicator lines on both sides are at 0 (Figure 3A).
- Use the medial-lateral and anterior-posterior knobs on the head holder (Figure 2) to center-align the ear bars in the x- and y-planes above the crosshair of the center height gauge (Figure 3A).
- To align the ear bar position in the z-axis, remove the ear bars from the holder and remove the center height gauge. Replace the ear bars and center them again at 0.
- Sight down the scope. Use the vertical shift knob (Figure 3B) and coronal tilt knob, respectively, to lower and rotate the ear bars until the scope crosshairs remain centered between the ear bars throughout coronal rotation.
- The stereotax is now calibrated and ready. Do not make any further adjustments to the position of the head holder.
3. Preparation of materials for injection/implantation
- Ensure that all instruments, surgical tools, and materials are sterilized and placed in a sterile surgical field next to the stereotax.
- Handle and store viral constructs according to their biosafety level and relevant institutional biosafety regulatory requirements.
- Draw up the virus into the syringe, taking care to use proper handling practices and personal protective equipment.
4. Anesthesia
- Record the mouse’s body weight prior to surgery.
- Deeply anesthetize the mouse using isoflurane.
- Ensure that the mouse is deeply anesthetized by performing a toe pinch test until the flinching response is absent. If the animal continues to show strong reflexes, increase the concentration and/or duration of anesthesia.
- Apply eye ointment to each eye to keep them moist during surgery.
- Shave the scalp from just behind the ears to just behind the eyes with a hair clipper.
- Provide the mouse with IACUC-approved analgesic.
- Continuously monitor the animal throughout the surgical procedure and provide thermal support.
5. Surgical procedure
- Place the head into the head holder by placing the upper incisors into the gap in the bite bar, making sure that the tongue is below the bite bar.
- Secure the head in the ear bars by gently inserting the ear bars into the external auditory meatus, ensuring that the ear bars are symmetrically placed (typically between three and four for an adult mouse). This step is critical to ensure the head is stable and centered for rotation.
- Aseptically prepare the shaved incision area with three alternating scrubs of betadine and alcohol swabs, or with alternative institutionally approved surgical site preparation.
- Place a surgical drape over the animal to maintain a sterile surgical field and to reduce the risk of post-operative infection.
- Expose the skull by making an incision along the sagittal midline of the scalp. Gently scrape the surface of the skull to remove any fascia and expose the sutures.
NOTE: If suture lines are difficult to visualize, hydrogen peroxide can be applied to the skull using a sterile cotton-tipped applicator to improve suture visualization. - Place the centering scope into the holder and center the crosshairs on bregma (Figure 4, left panel). Zero the micromanipulator.
- Move the crosshairs caudally to lambda, noting the bregma-lambda (B-L) distance.
NOTE: If the suture lines do not follow a straight line along the midline, it is recommended to establish the midline using the “line of best fit” through both bregma and lambda. However, if the above steps are followed, the initial placement of the scope reticle should be halfway between the ear bars and closely approximate the B-L midline suture. - If the B-L distance is significantly less or greater than 4.21 mm, incrementally adjust the assigned bregma to obtain a B-L distance of 4.21 mm ± 0.2 mm.
- Replace the centering scope with the alignment indicator. Place the probes on lambda and bregma and adjust the dorsal tilt knob on the head holder to level in the sagittal plane (nose facing up or down), then use the centering scope to reassign bregma.
- Use the alignment indicator to level in the coronal plane using the coronal tilt knob. Measure at multiple points throughout the rostral/caudal axis to account for surface deformations in the skull.
- Note the position on the dial of the coronal tilt knob, as this is the 0° rotation position.
6. Aligning the central axes of rotation for angled coordinates
- Secure the centering scope in the tool holder and position the micromanipulator to the calculated coordinate from section 1. Note that the R/L coordinate for the angled implantation corresponds to the length of side A.
- In the example in Figure 1, the angled coordinates for fiberoptic placement targeting the VMN are (A/P = -1.4, R/L = [2.03] at 0° coronal rotation, [0.00] at 15° coronal rotation, D/V = -5.4).
- Sighting down the scope and mark this coordinate (R/L 2.03 mm from the midline per the VMN example; Figure 4, middle panel). This mark represents the point at which the cannula will enter the brain once the head is rotated.
- Reposition the micromanipulator over the midline (R/L = 0.00). Use the coronal tilt knob to rotate the head to the angle calculated in section 1.
- If the scope crosshairs already line up with the mark, proceed to section 7.
- If the scope crosshairs do not line up with the reference mark, adjust the head position in the z-axis using the vertical shift knob (Figure 2) until the crosshairs line up as close as possible to the mark.
- Rotate the head back to the 0° coronal position. If the vertical shift was adjusted in step 6.3, reassign bregma using the centering scope.
- Repeat steps 6.3 and 6.4 until the crosshairs consistently hit the reference mark when the head is rotated (Figure 4C).
- At this point, the arbitrary point of rotation established in section 1 should now be aligned with the stereotactic center of rotation.
7. Microinjection
- Place the stereotactic drill in the holder and maneuver the micromanipulator to the first injection coordinate.
- Per the example for targeting the VMN, drill at A/P = -1.4 and R/L = 0.4 while the head is level.
- Lower the drill until the bit is just above the skull. Turn on the drill, and gently lower until the bit has just drilled through the skull (not the dura).
- Repeat for the contralateral injection site.
- Use a sterile needle-driver to introduce a 90° bend into a 27-30G needle (e.g., of a sterile 0.5 mL insulin syringe), and use the bent needle to gently poke through the dura mater.
- NOTE: If bleeding occurs, apply pressure with a sterile cotton-tipped applicator and clean with sterile water until the bleeding has stopped.
- When ready to inject, carefully place a filled Hamilton syringe into the stereotactic holder.
NOTE: The coordinates on the micromanipulator no longer apply after switching to a new tool. Use the center of the burr hole as the new target for injection. - Carefully position the needle above the burr hole.
- Lower the needle until it slightly touches the dura within the center of the burr hole. CRITICAL: Zero the micromanipulator only in the z-axis, such that the coordinates on the micromanipulator for the stereotactic centering scope and drill are maintained.
- Slowly lower the needle into the brain, watching closely to ensure that the needle does not deflect on the edge of the burr hole. Continue to lower until 0.05 mm ventral to the D/V injection coordinate and wait 1 min. This extra step creates a small “pocket” to minimize viral backflow on needle removal.
- Slowly raise the needle to the D/V coordinate and start the injection.
NOTE: Flow rate and volume will vary depending on target region and experimental design. For optogenetic silencing of VMN neurons, sufficient coverage is desired, so 200 nL of virus is injected at a rate of 1 nL/s. - Following microinjection, wait 10 min at the injection site to minimize efflux of virus during withdrawal.
- Slowly withdraw the micropipette from the brain at an approximate rate of 1 mm/min.
- Once the needle is clear of the skull, eject a small volume of virus to ensure the needle has not clogged with blood or tissue. Use a sterile cotton-tipped applicator to remove the virus before continuing.
- Repeat steps 7.6–7.12 for the contralateral side.
- Seal the microinjection burr holes with bone wax to improve healing (Figure 5B).
8. Fiberoptic implantation
NOTE: After viral injection, bilateral fiberoptic cannulas are implanted at the calculated angle per section 1. Note that these coordinates should already be marked on the skull from section 6.
- Repeat steps 7.1 –7.4 for the angled coordinates.
- Return the head to the level 0° position.
- Next, use the hand drill to produce four additional holes for the bone screws: two should be placed anteriorly and two posteriorly (Figure 5A). These will serve as anchors to affix the fiberoptics to the skull (Figure 5D).
NOTE: Make sure to space the holes far enough away from the angled coordinate burr holes to accommodate the ferrule portion of the fiberoptic that sits above the skull. - As gently as possible, use the small flathead screwdriver to set the bone screws such that they sit firmly in the skull but do not penetrate the brain.
- Clamp a fiberoptic cannula into the cannula holder and place it in the stereotactic holder.
- Rotate the head to the calculated angle, noting again that the coordinates on the micromanipulator do not apply to the new tool. Use the center of the angled burr holes as the implantation target.
- Lower the fiberoptic until it just touches the dura within the center of the burr hole (Figure 5C). Zero the micromanipulator in the z-axis, then slowly slower the fiberoptic to the D/V angled coordinate (-5.4 per the VMN example).
- Use cyanoacrylate gel to connect the fiberoptic ferrule to the ipsilateral anchor screws, then apply an accelerant with a micropipette tip (Figure 5D).
- Once the cyanoacrylate gel has completely hardened, gently loosen the cannula holder and raise until clear of the fiberoptic ferrule.
- Repeat steps 8.5–8.9 for the contralateral angled coordinate, then level the head. For extra security, make an additional connection between the two angled fiberoptic cannulas with the cyanoacrylate gel and accelerant (Figure 5D).
- Prepare a small, relatively thin amount of dental cement. Apply to the surface of the skull, making sure to thoroughly cover the anchor screws and base of the fiberoptic cannulas. Leave enough of the ferrule clean for subsequent mating with the fiberoptic patch cables.
- Once the cement is completed dry, remove the mouse from the stereotactic apparatus.
- Place mouse in a recovery cage with thermal support. Allow it to recover and transfer to the home cage once it appears alert, mobile, and is grooming.
9. Post-surgical care
- Monitor animals daily for 3 days post-operatively for behavior, posture, activity, and grooming, and keep records of food intake and body weight.
- If animals exhibit any general indicators of pain or poor health, consult with veterinarian services.
- Allow mice at least 2 weeks for recovery and for viral expression before starting behavioral studies.
10. Optogenetics
- For the performance of optogenetics studies, refer to Sidor et al.8.
- Validate viral expression and fiber placement at the completion of studies.
This protocol describes a surgical procedure for performing optogenetics studies to interrogate the role of hypothalamic VMN neurons in glycemic control9. First utilized was a standard (non-angled) stereotactic approach for the bilateral microinjection of an inhibitory channelrhodopsin virus to the VMN. While an angled approach would also be suitable, the standard (non-angled) approach was selected because it is sufficient to target the brain region of interest and is an easy, reliable and consistent approach. However, given the VMN’s proximity to the midline, space constraints did not permit the non-angled implantation of bilateral fiberoptics, necessitating the development of a surgical strategy for precisely implanting fiberoptics at an angle (Figure 6).
Using this surgical strategy, we microinjected a Cre-dependent AAV expressing a modified channelrhodopsin anion-conducting channel fused with the fluorescent reporter, referred to as a ”SwiChR++” virus10, bilaterally to the VMN of Nos1-cre mice. This was followed by implantation of an optic fiber dorsolateral to each injection site at a 15° angle from the midline. As expected, viral expression was restricted to the VMN and not detected in other brain areas.
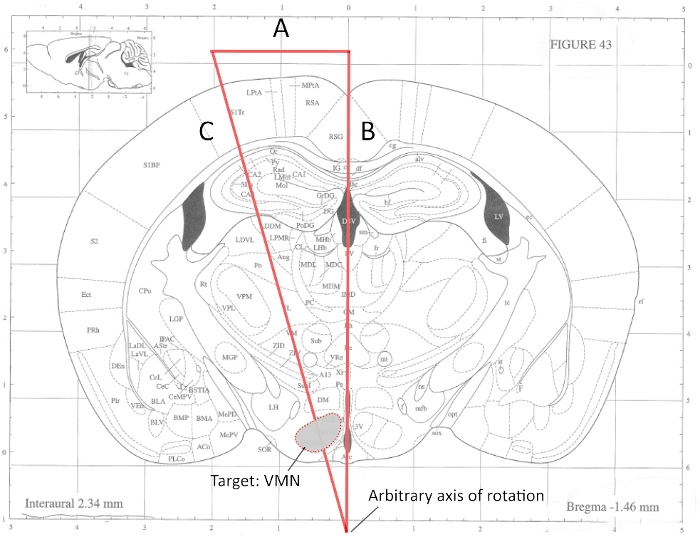
Figure 1: Representative example of calculating angled coordinates targeting the hypothalamic ventromedial nucleus. Angles and line segments are not drawn to scale. (A) This length should be calculated using basic trigonometry. In this example, A = 2.03 mm. (B) Estimated length based upon assignment of arbitrary axis of rotation. In this example, B = 7.576 mm. (C) Calculated hypotenuse. It should be noted that the depth of fiberoptic/needle insertion depends upon the desired proximity to the target region, which requires optimization. This figure has been modified from Faber et al. 201911. Please click here to view a larger version of this figure.
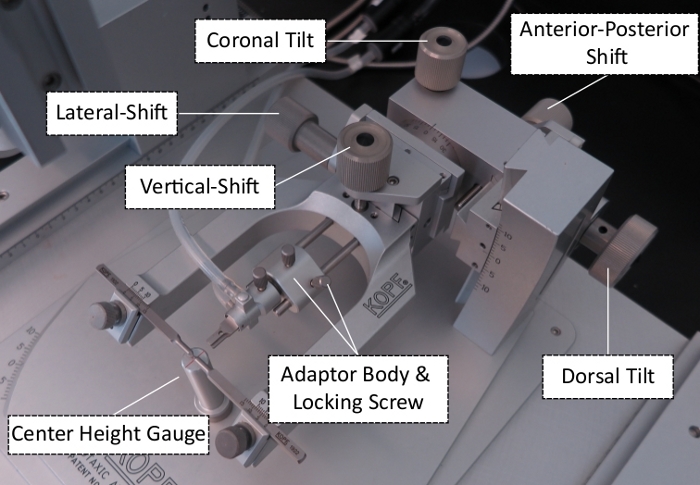
Figure 2: Adjustment knobs for the stereotactic head holder apparatus. This figure has been modified from Faber et al. 201911. Please click here to view a larger version of this figure.
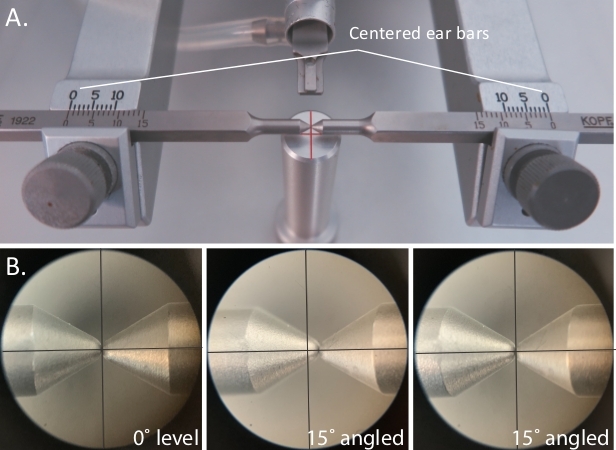
Figure 3: Aligning the head holder center of rotation. (A) Positioning the ear bars. (B) Sighting down the scope during 0° level coronal rotation (left), during 15° rotation before adjusting the vertical shift, and the center of rotation is misaligned (middle), and during 15° rotation after adjusting the vertical shift, and the center of rotation is properly aligned (right). This figure has been modified from Faber et al. 201911. Please click here to view a larger version of this figure.
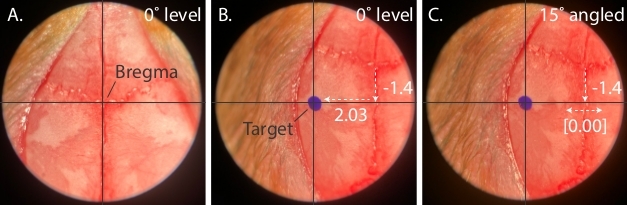
Figure 4: Assigning bregma and aligning the animal head with central axes of rotation. (A) Representative image indicating typical bregma placement. (B) Drawing a reference mark while head is level, before alignment. (C) Properly aligned axis of rotation, after adjusting the vertical shift and readjusting bregma. Please click here to view a larger version of this figure.
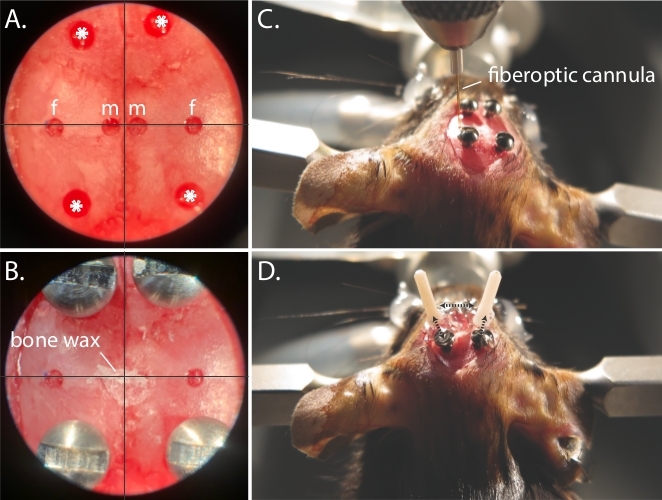
Figure 5: Fiberoptic implantation procedure. (A) Centering scope view of pilot holes for microinjection (m), fiberoptic (f), and anchor screws (*). (B) Centering scope view of implanted anchor screws, and bone wax covered microinjection drill holes. (C) Positioning the fiberoptic into place during angled implantation. (D) Representative bilateral angled fiberoptic placement. Dotted black arrows indicate areas in which super glue is used to anchor the fiberoptic to the anchor screws and ipsilateral fiberoptic. Please click here to view a larger version of this figure.
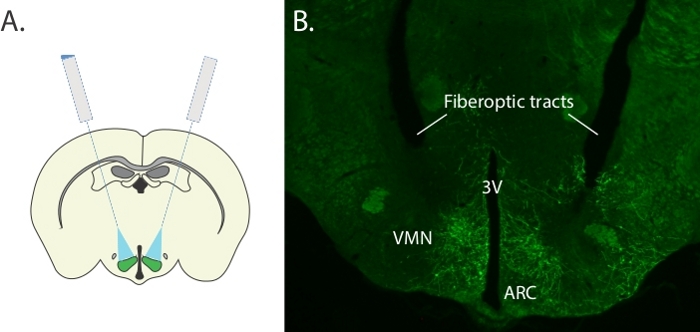
Figure 6: Representative results for bilateral targeting of the ventromedial hypothalamus. (A) Schematic representing bilateral microinjection and angled fiberoptic strategy for targeting the VMN. (B) Representative image showing bilateral expression of SwiChR-GFP and tissue damage from angled fiberoptic tracts. 3V = third ventricle, ARC = arcuate nucleus, and VMN = ventromedial nucleus. Please click here to view a larger version of this figure.
