Surgical Operation Time
After training, a skilled surgeon can successfully perform the operation within 35 minutes using the inner tube technique, wherein approximately 15.5 minutes are required for recipient preparation, 10.9 minutes are required for donor preparation, and 4.4 minutes are required for donor heart anastomoses. The cold and warm ischemia time (from donor preparation to heart implantation) is reduced to 15.3 minutes compared to the operation using the cuff technique without the inner tube technique and suture technique (Table 1)21.
We designed a cooperation model to further improve the efficiency of the operation. As shown in the schematic (Figure 3), one surgeon begins performing recipient preparation first, followed by initiation of the donor preparation by a second surgeon after 4-5 minutes. After 15-16 minutes, the first surgeon should have finished the recipient preparation, at which point the second surgeon having finished harvesting the donor heart, should begin anastomosing the donor heart within the recipient. This cooperation model requires each surgeon to be trained in only a single part of the cuff technique and further shortens the total operation time to approximately 25 minutes. An analysis of >600 heterotopic murine transplantations performed via cooperation between two surgeons over the past two years at the Organ Transplantation Institute of Xiamen University indicates a success rate for cardiac transplantation using this technique of up to 95%.
Survival of Major Histocompatibility Complex Cardiac Mismatched and Matched Cardiac Grafts
Major Histocompatibility Complex (MHC), designated “H-2”, has been used to determine genetic disparities and similarities. Donor-mismatched MHC antigens can trigger graft rejection by interacting directly with the recipient T cells or indirectly as donor MHC-derived peptides expressed on recipient MHC molecules23. A fully MHC mismatched BALB/c (H-2d) allograft heart can be rejected, with a median survival time of 7.5 days after transplantation into C57BL/6 (H-2b) recipient mice (Figure 4A). In our studies, syngeneic heart transplants survived more than 100 days, except in one rare case due to a 15% weight loss compared to normal weight before the operation.
Heart allografts can be harvested for histopathological examination at the time of rejection. Figure 4B shows the appearance of marked cell-mediated rejection characteristics, such as inflammatory cell infiltration, tissue edema, and microvascular occlusion. Syngeneic grafts are near normal with no evidence of myocyte necrosis or inflammatory cell infiltration.
Effect of Inner Tube on Vascular Endothelium
To evaluate the damage on the vascular endothelium after inserting the inner tube into the lumen, 100 days after syngeneic heart transplant, the vascular endothelium of anastomosis site can be collected and stained by immunofluorescent. In this analysis, no obvious narrowing of vascular wall, thrombosis, or thickening of the intima were observed (Figure 4C). Electron microscopic imaging revealed that a smooth endothelium and a regular longitudinal crest formation, with the endothelial cells arranged neatly and closely, with no obvious sediments on the surface (Figure 4D).
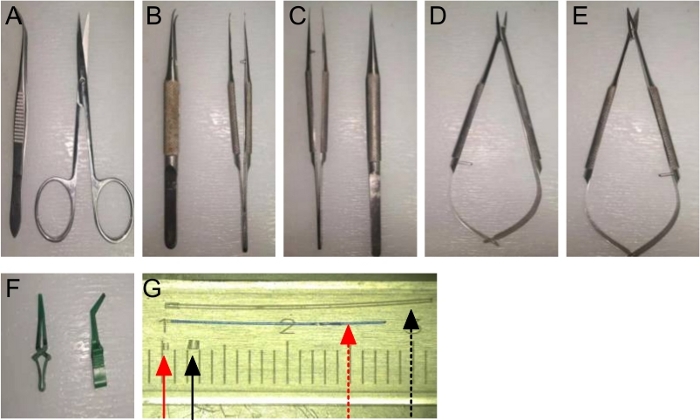
Figure 1: A set of Sterile Surgical Instruments:
(A) Fine forceps and ophthalmic scissor; (B) Micro curved forceps; (C) Micro straight forceps; (D) Micro needle holders; (E) Micro scissors; (F) Bulldog clamps; (G) An artery inner tube (red dotted arrow) and cuff (red solid arrow), along with a vein inner tube (black dotted arrow) and cuff (black solid arrow). Please click here to view a larger version of this figure.
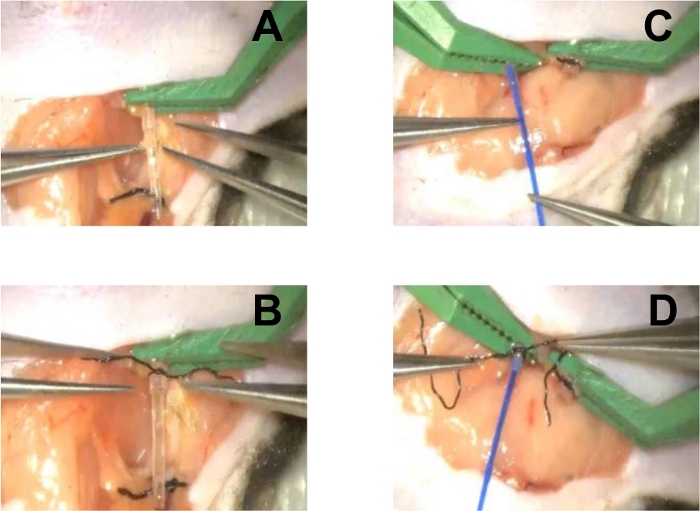
Figure 2: Recipient Preparation.
(A) Insert the vein inner tube into the external jugular vein vessel; (B) Evert the vein vessel over the cuff and fix it using a circumferential 8-0 silk suture; (C) Insert the artery inner tube into the lumen of the artery vessel; (D) Evert the vein vessel over the cuff and fix it using a circumferential 8-0 silk suture. Please click here to view a larger version of this figure.
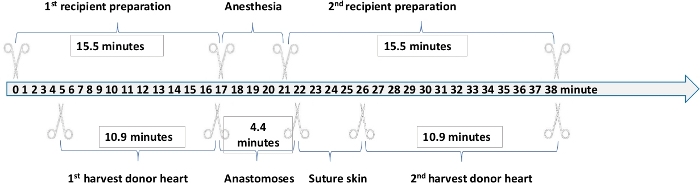
Figure 3: Operation Time of Each Step in Heterotopic Murine Transplantation. Please click here to view a larger version of this figure.
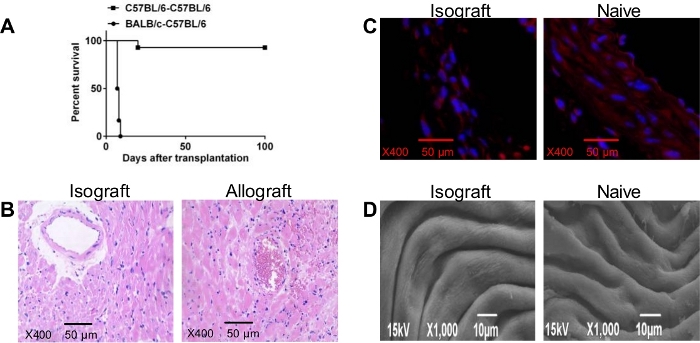
Figure 4: (A) Cardiac graft Survival Time. Kaplan-Meier plot displaying the survival of heart allografts (BALB/c) and syngeneic grafts (C57BL/6) from donor mice transplanted into C57BL/6 recipient mice (n=12 mice/group); (B) Microscopic Examination of C57BL/6 (left) Isograft and Wild Type BALB/c Allograft (right) on Day 7 after Transplantation (Scale bars, 50 um; magnification ×400); (C) Immunofluorescence (Scale bars, 50 µm; magnification ×400) (D) Electron Microscopy Scanning of Vascular Endothelium in Transplant (left) and Naive (right) Recipient. Please click here to view a larger version of this figure.
| Anastomosis technique | Recipient preparation time | Donor preparation time | Heart implantation time | Cold and warm ischemia time | Total operation time | |
| 5Cervical Heterotopic | Suture | N | N | N | < 45 min | N |
| 6Cervical Heterotopic | Cuff | 45 min | 15 min | 10 min | N | N |
| 24Cervical heterotopic | Cuff | 15 min | 20 min | 15 min | 25-40 min | < 60 min |
| 25Abdomen Heterotopic | Suture | N | N | N | N | 35 min |
| 7Cervical Heterotopic | Cuff | N | 20 min | N | 30 min | 35 min |
| 26Cervical Heterotopic | Cuff | N | 20 min | 20 min | < 35 min | N |
| 4Abdomen Heterotopic | Suture | 60–70 min | 6–7 min | N | N | 75 min |
| 21Cervical Heterotopic | Cuff | N | N | 7 min | 20 min | 45 min |
| 27Abdomen Heterotopic | Suture | N | 10-15 min | N | N | 45-60 min |
| 28Cervical Heterotopic | Cuff | 25 min | 20 min | 15 min | 20 min | 60 ± 8 min |
| 29Cervical Heterotopic | Cuff | 31.9 min | 21.1 min | 5.1 min | 28.5 min | 57.8±3.9 min |
| 29Cervical Heterotopic | Suture | 25.2 min | 20.5 min | 30.8 min | 51.3 min | 83.9±2.9 min |
| Cervical Heterotopic in Our Protocol | Cuff | 15.5 min | 10.9 min | 4.4 min | 15.3 min | 35 min |
| (Single Operation) | ||||||
| 23 min | ||||||
| (Cooperation) |
Table 1: Comparison of Time of Different Phases in Different Mouse Heart Transplantation Techniques.
