The described FUS system (Figure 1 and Figure 2) and the associated workflow have been used in over a 100 animals and produced reproducible data on both healthy and tumor bearing mice. Based on the recorded cavitation and the spectral density at the harmonics at the peak moment of the microbubble bolus injection, the spectral power of each frequency can be calculated using the Fourier analysis as explained in step 4 of the Protocol. Based on the acoustic protocol (1 MHz, 10 ms pulse duration) with a MI of 0.4 in combination with microbubbles, the normalized integrated power spectrum at the 2nd and 3rd harmonics normalized the integrated power spectrum of the excitation frequency observed in Figure 3. This provided a very sensitive and reliable means of stable cavitation detection, in comparison to no detection of subharmonics when no microbubbles were injected or the observation of inertial cavitation when a MI of 0.6 was applied. In case of inertial cavitation, an increased broad-band noise floor of up to 25 dB was detected as well as the appearance of ultra-harmonics and subharmonics. Although an acoustic pressure of an MI of 0.4 and 0.6 resulted in no macroscopic damage, microscopic damage was evidenced histologically at a MI of 0.6, as shown in Figure 4. A further increase of the pressure amplitude up to a MI of 0.8 resulted in a macroscopic brain hemorrhage of larger vessels and wide-spread tissue lysis with the extravasation of erythrocytes. The histological findings corresponded to the acoustic data from the passive cavitation sensor, as shown in Figure 3, confirming the damaging properties of inertial cavitation of the brain tissue. As a consequence, a MI of 0.4 was chosen as the safe pressure amplitude that provided very reproducible BBB-opening, while providing a safe margin to the inertial cavitation regime, as observed before11.
Intravenous Evans blue was injected to validate the opening of the BBB in the pontine region. The strong albumin-binding of Evans blue leads to a large molecule of more than 66 kDa42. At the level of the pons and partly the cerebellum, extravasation of Evans blue-conjugated albumin was observed in the mouse treated with FUS and microbubbles in contrast to the mouse without microbubbles (Figure 5). This emphasizes the precise targeting of the region of interest based on image-guided stereotactic navigation with the in-house build FUS system and the described protocol.
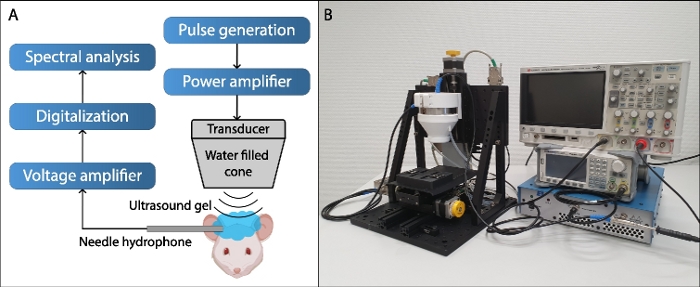
Figure 1: Focused ultrasound setup.
(A) Schematic representation of the focused ultrasound set up. (B) Picture of the focused ultrasound setup. The system consists of a top-down mounted transducer on a 1D linear stage over a second 2D stage for automatic 3D positioning. The transducer is built in a water filled beam-cone, closed at the bottom with an acoustically transparent mylar membrane, which conducts the sound to the cranium of the animal. The transducer is connected to a power amplifier, which is in-turn connected to an arbitrary waveform generator (AWG) for signal generation. For cavitation detection a detachable hydrophone in combination with a low-noise voltage amplifier is used. The hydrophone is placed in the direct vicinity of the occipital bone. The external hydrophone has a 2 mm active surface and is acoustically coupled with ultrasound gel. Both the high-voltage signal of the excitation pulse as well as the recorded cavitation signal are digitalized by a standard 200 MHz oscilloscope and relayed to a control computer (not shown) for on-the-fly processing and real-time control. Please click here to view a larger version of this figure.
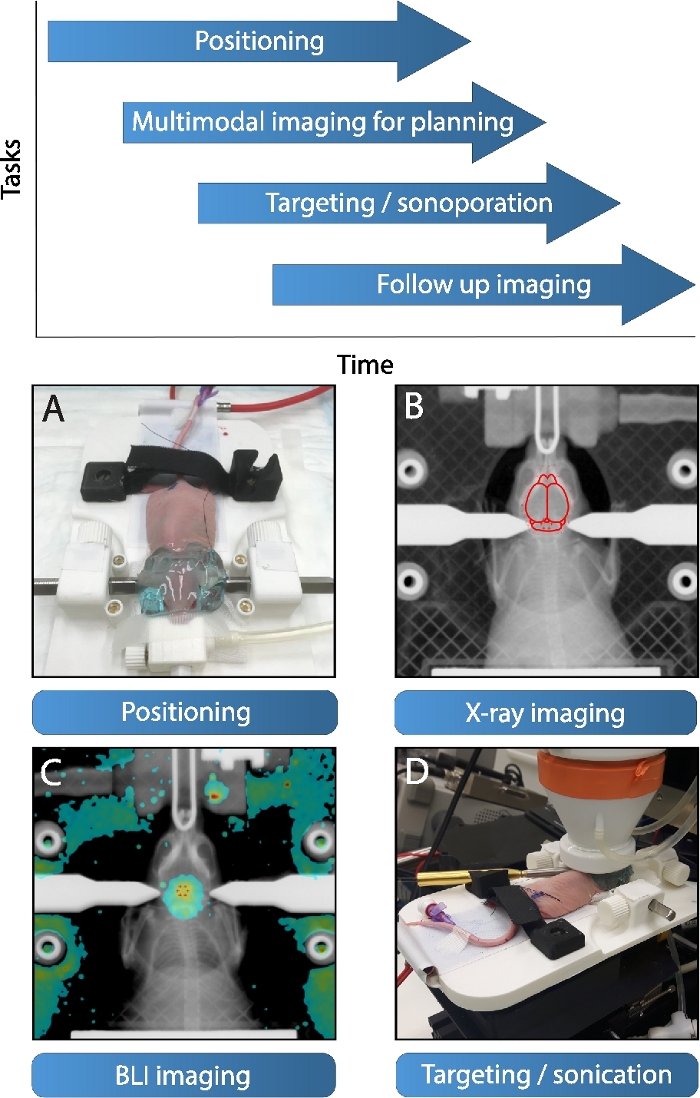
Figure 2: Focused ultrasound workflow.
The proposed workflow of the focused ultrasound system starts with (A) the initial positioning of animal on a detachable stereotactic platform, note the application of the acoustic coupling gel (applied post BLI/X-ray). Simultaneously multimodal imaging can be conducted for targeting. (B) At first X-ray imaging is a possibility, whereas a region of interest can be targeted with the help of an outline of the brain (which in turn is referenced to the mouse brain atlas40, adapted to the size and posture of the skull). (C) Alternatively, a BLI image of a luciferase transfected diffuse midline glioma tumor overlaid on an X-ray maximum intensity projection can be applied for targeting. (D) Subsequently, the stereotactic platform is mounted with the animal in therapy position with both hydrophone and transducer attached. The transducer automatically drives in therapy position and sonicates the chosen trajectory post bolus injection. The system is optimized for high-throughput experiments, whereby multiple platforms allow interleaved work, as shown on top. Please click here to view a larger version of this figure.
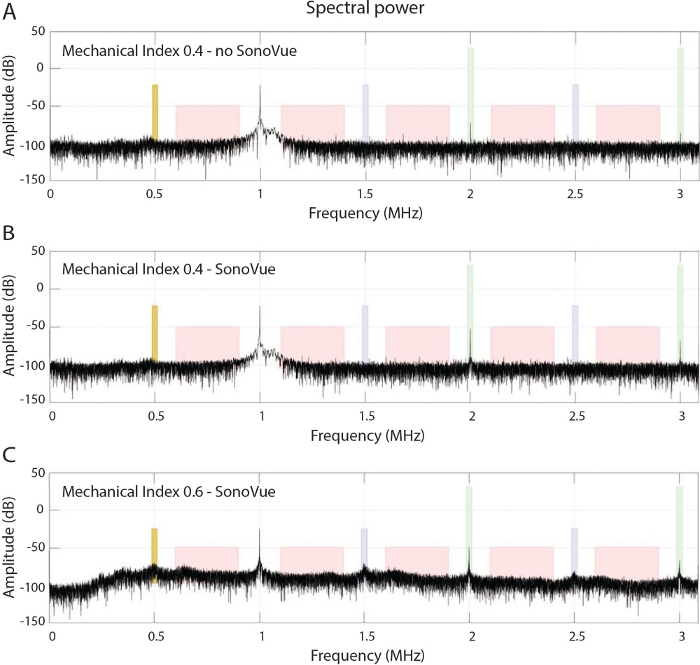
Figure 3: Cavitation monitoring.
(A) Frequency spectrum of an in vivo experiment in the absence of microbubble administation at a MI of 0.4 at 1 MHz. (B) Shown is the corresponding spectrum at peak-bolus after injection of microbubbles. Note the increase of the higher harmonics, which is indicative for stable cavitation of the microbubbles. (C) Corresponding spectrum observed at a higher MI of 0.6 in combination with microbubble injection, within the transition band to the onset of inertial cavitation, leading to an increase in noise floor up to 25 dB and the appearance of ultraharmonics and subharmonics. Please click here to view a larger version of this figure.
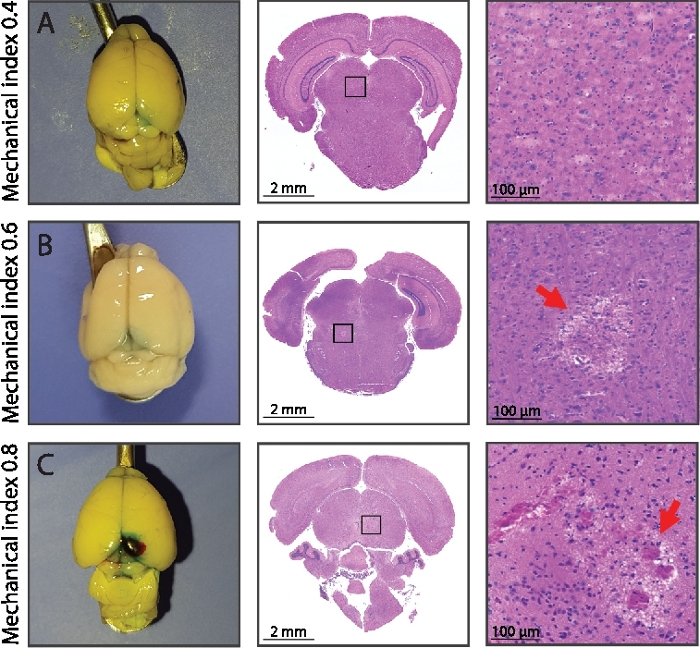
Figure 4: BBB opening and associated histology.
(A) Stable cavitation using an MI of 0.4 evidenced an intact brain parenchyma in both white light macroscopy and HE stained microscopy. (B) After a MI of 0.6 first signs of local irreversible tissue damage of the brain parenchyma is becoming apparent in the HE stained histological data. (C) For even higher mechanical pressure of MI 0.8, macroscopic hemorrhaging is apparent as well as wide-spread tissue lysis of the brain parenchyma and the extravasation of erythrocytes due to micro-hemorrhaging. The blue hue in the white light macroscopy is indicative for the extravasation of the co-injected intra-vascular contrast agent Evans blue indicating BBB opening (see Figure 5 for a sagittal view). Please click here to view a larger version of this figure.
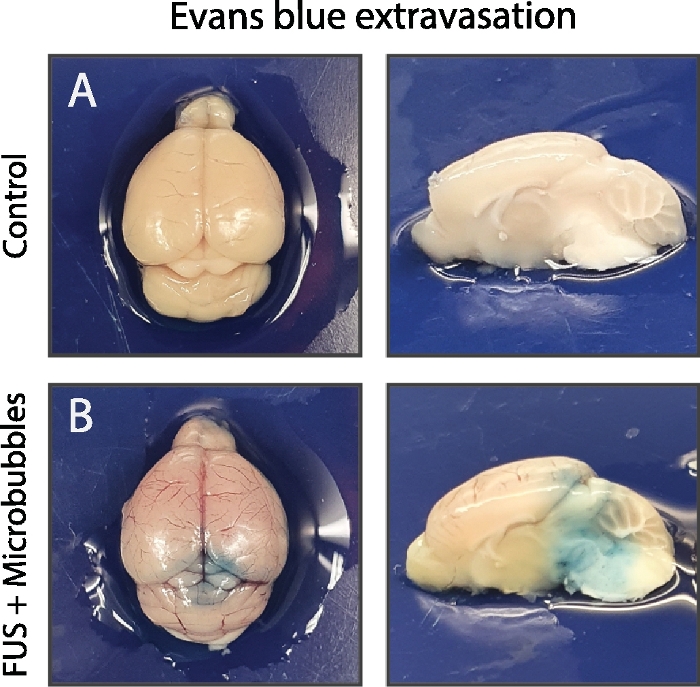
Figure 5: Validation of BBB opening.
Demonstration of successful BBB opening in the stable cavitation regime (B) compared to the control (A), no microbubbles injected. In this case Evans blue has been used as an intravascular contrast agent. The strong albumin-binding of Evans blue leads to a large molecule of more than 66 kDa. As a consequence, evidence of the Evans blue extravasation is indicative for paracellular transport across the BBB due to a (partial) opening of the tight junctions. Please click here to view a larger version of this figure.
