Here we present in detail a protocol that has previously been described31 and used11,12,13,14,15,16,17,18 to measure the capacity of antibodies targeting the surface of P. falciparum IEs to induce opsonization and phagocytosis by THP-1 cells.
The assay specifically measures antibody-mediated phagocytosis and, therefore, interaction with the appropriate Fc-receptors on the surface of the THP-1 cells is required. For this reason, and as mentioned in the protocol, we recommend periodically checking the expression of Fcγ-receptors on the surface of the THP-1 cells by flow cytometry. The cells should be negative for CD16 (Figure 1A) and positive for CD32 and CD64 (Figure 1B,C).
For the assay, purified late-stage IEs were labeled with EtBr and then opsonized with antibodies present in the plasma/serum of malaria-naïve or malaria-exposed individuals. Phagocytosis was measured by flow cytometry, quantifying the percentage of EtBr+ THP-1 cells after 40 min co-incubation with EtBr-labeled and antibody-opsonized IEs. Initially, THP-1 cells were gated using an FSC vs. SSC density plot (Figure 2A). Then, an EtBr+ marker was created, using an FL3 histogram on the THP-1 cells and un-opsonized IEs (Figure 2B). These gates were then used to analyze all the other controls and test samples.
The negative controls (including the THP-1 cells alone, the un-opsonized IE control, and the controls with malaria-naïve and malaria-exposed males) should all generate a single negative peak in the FL3 channel (Figure 3A) with only few events in the EtBr+ marker. Accordingly, the mean phagocytosis values both as absolute EtBr+ THP-1 cells and as relative phagocytosis percentages should be very low (Figure 3B,C, normally less than 2% for all cases). In contrast, the positive controls (including the rabbit anti-human erythrocyte antibody and the malaria-exposed female pool) should generate traces with two peaks (Figure 3A): a negative one (largely overlapping with the one generated by all the negative controls) and a clearly positive and well-separated one located inside the EtBr+ marker. A positive sample, as the presented example (sample from a malaria-exposed multigravid woman/NF20) should generate a similar profile as the positive controls. The mean phagocytosis values, measured as absolute EtBr+ THP-1 cells and as relative phagocytosis, were normally highest for the positive control (58%/100%), followed by the malaria-exposed female pool (29%/53%), and then the single malaria-exposed woman (23%/40%). As observed in Figure 3B,C, where three independent experiments are presented, there was a considerable variability between experiments and we, therefore, recommend running samples intended for comparison in the same experiment. In our hands, at least four full 96 well plates can be handled by a single experienced researcher. The variability between assays was also clearly observed when two identical experiments testing several serum samples from malaria-exposed women were performed simultaneously. The same parasite preparation (after magnetic purification of late-stage IEs) and serum dilutions were used. THP-1 cells were kept in two separate flasks but seeded from the same initial flask and the experiments were performed by two different researchers. Even though the assay seems to generate consistent results when performed separately, with tight linear correlations (r>0.9 for both absolute and relative phagocytosis values) between phagocytosis values measured in the two experiments, the slope coefficient of the adjusted lines deviates from one, indicating the values generated in different experiments were not identical. This deviation was more evident for the absolute values (slope coefficient confidence interval 0.55-0.72) as compared to the relative values (slope coefficient confidence interval 0.68-1) (Figure 4). We, therefore, recommend using relative values, especially if for some reason (e.g., not enough purified IEs, more than 4 full plates, etc.) it is not possible to run all the samples in a single experiment. We also recommend running experiments intended for comparative analysis within the shortest amount of time, to avoid introducing extra variation due to drifting in PfEMP1 expression (as well as other antigens) and due to subtle differences on the THP-1 cells upon extended time in culture.
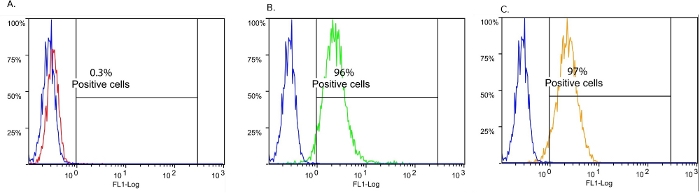
Figure 1: Fc receptors expressed on the THP-1 cell surface.
(A) Fcγ-receptor III/CD16 (red). (B) Fcγ-receptor II/CD32 (green). C. Fcγ-receptor I/CD64 (orange). Un-labeled cells are shown in blue. Please click here to view a larger version of this figure.
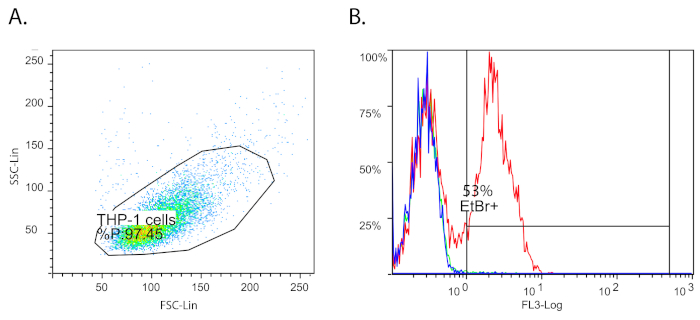
Figure 2: Flow cytometry gating strategy.
(A) THP-1 cells gated on FSC/SSC. (B) Ethidium bromide positive (EtBr+) THP-1 cells in an FL3 histogram. THP-1 cells alone/no IEs added (blue), THP-1 cells incubated with un-opsonized IEs (green), and THP-1 cells incubated with IEs opsonized with a positive control (red) are shown. Please click here to view a larger version of this figure.
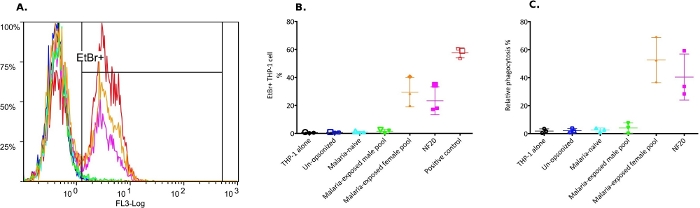
Figure 3: Phagocytosis of IT4VAR04-IEs by THP-1 cells.
(A) Representative flow cytometry histograms of one of the experiments presented in B (identified by larger symbols). (B) Percentage of EtBr+ THP-1 cells (means and standard deviations of three independent experiments). (C) Same data as in B, after normalization against the corresponding positive control. Color coding is the same in all panels: THP-alone (black), un-opsonized/no antibody control (blue), malaria-naïve control (cyan), malaria-exposed male pool (green), malaria-exposed female pool (orange), a malaria-exposed female donor (pink), and positive control/rabbit anti-human erythrocytes (red). Mean and standard deviations are shown. Please click here to view a larger version of this figure.
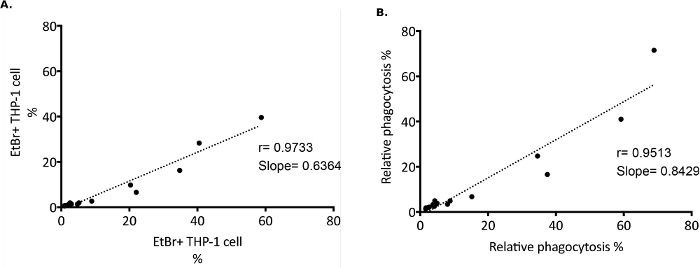
Figure 4: Phagocytosis of IT4VAR04 IEs by THP-1 cells upon opsonization with serum from 10 malaria-exposed women.
The plots present linear regression analysis for two identical experiments performed on the same day, but by different researchers. (A) Data presented as absolute values and as (B)relative phagocytosis values. Analysis performed using statistical analysis software. Please click here to view a larger version of this figure.
Figure S1: Phagocytosis assay flow chart. Flow chart depicting the main steps of the assay. Please click here to download this figure.
Figure S2: 96 well plate experiment layout. (A) Layout for IEs EtBr labeling. (B) Layout for opsonization; 6 wells are always reserved for controls. (C) Layout for THP-cells plating. (D)Layout for phagocytosis. Please click here to download this figure.
Figure S3: Color coding as in Figure 3. (A) Flow cytometry histogram overlay of one experiment acquired immediately and (B) after storage at 4 °C for 12 h. (C) Percentage of EtBr+ THP-1 cells measured before and after storage. NF## represent different malaria-exposed female donors. Please click here to download this figure.
