Our group has several years of experience with solid organ transplantation models in small- and large animals and utilized the porcine orthotopic kidney auto-transplantation model, obtaining reproducible results in various experimental settings16,25,26,27. Depending on the experimental setup, we recommend performing 3 to 5 auto-transplantations as preliminary experiments which ensures a sufficient learning curve of the whole experimental team. In the present setting 5 transplantations were required to train a surgeon, with 8 years of previous experimental- and 5 years of clinical surgical experience in the field of transplantation surgery, in performing these experiments. This can differ depending on the previous exposure of the surgeon to these techniques.
Within the frameworks of this protocol, the results of a set of 5 porcine orthotopic kidney auto-transplantation experiments are demonstrated. Transponder implantation was successful in each animal with sufficient telemetry signals throughout the observation period (except one animal with partial transponder dysfunction). Knife-to-skin interval for the transponder implantation was 85 min ± 5 min (Table 1). Following graft retrieval, all animals recovered well in the housing facility. Knife-to-skin interval for the retrieval surgery was 135 min ± 32 min (including approximately 30-45 min for the insertion, tunneling and securing of the jugular catheter). The left kidney was stored in a cold water-bath with a target cold ischemia time of 24 h (24 h ± 30 min). The following day, after anesthesia induction and relaparotomy, the contralateral (right) kidney was removed followed by the orthotopic auto-transplantation of the cold stored left kidney graft as described earlier. Knife-to-skin interval for the auto-transplantation surgery was 168 min ± 27 min (including the explantation of the right kidney). Warm ischemia time was 34 min ± 7 min. Each implanted kidney graft had a minimal but direct urine production following reperfusion. Following abdominal closure, color Doppler ultrasound showed satisfactory arterial and venous perfusion of the kidney in all cases (Figure 4). All animals recovered from the anesthesia and no significant complications were observed throughout the observation period. Daily blood and urine samples were collected. All pigs were in good clinical condition during the follow-up and were sacrificed after 5 days. Serum creatinine and potassium values peaked on POD3-4. The blood pH has remained within normal ranges (Figure 5). Urine output recovered to normal values over the first four postoperative days. White blood cell count was slightly increased at the end of the follow-up period (Figure 5). Body temperature, measured by continuous telemetry monitoring, showed slight fluctuations over the postoperative period.
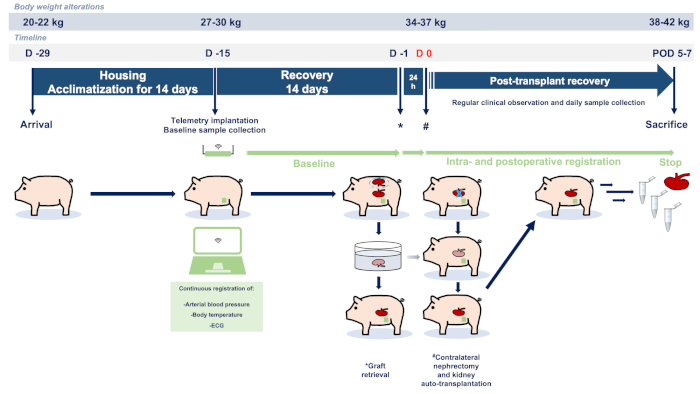
Figure 1: Study flowchart and protocol. Abbreviations used: POD-postoperative day; ECG-electrocardiography. Please click here to view a larger version of this figure.
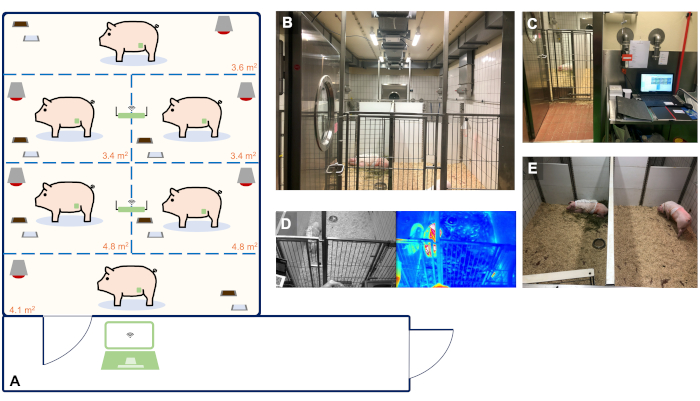
Figure 2: Animal housing facility with real-time and continuous telemetry monitoring of up to 6 animals. (A) Schematic blueprint of our facility suitable for the housing and telemetry monitoring of up to 6 animals. The size of the single holding boxes was determined based on the guidelines of the EU Directive 2010/63 and ETS 123 Appendix A. Panels A-E show representative images of the organization of our facility. (B) Animal room for the housing of 6 animals. (C) Observation room with a PC used for the continuous registration of telemetry data. (D) Real-time video and thermal footage of the animals. (E) Individual holding ensuring acoustic and olfactory contact of the animals with their companions to avoid social isolation. Please click here to view a larger version of this figure.
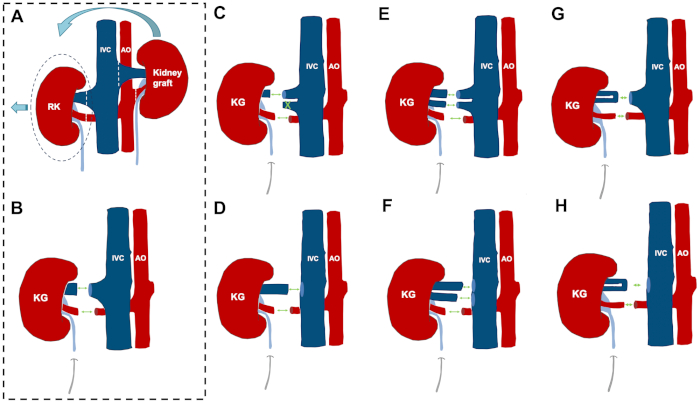
Figure 3: Orthotopic kidney auto-transplantation and anatomical variations and reconstruction possibilities. (A,B) The steps of the orthotopic kidney auto-transplantation model in case of a "standard" vascular anatomy. (C) Variation 1: while one larger vein comes with the donor kidney, there are two veins on the recipient side. Management: the smaller vein is closed by a ligature and the anastomosis is performed end to end between the renal veins. (D) Variation 2: while one larger vein comes with the donor kidney, there is no suitable recipient vessel on the contralateral side (e.g., size mismatch). Management: end to side anastomosis of the renal vein to the inferior vena cava. (E) Variation 3: two similar-sized veins on both sides. Management: reconstruction by two venous anastomoses. (F) Variation 4: while two similar-sized veins come with the donor kidney, there is no suitable recipient vessel on the contralateral side. Management: end to side anastomosis of the renal vein to the inferior vena cava in the case of two renal veins. (G) Variation 5: a donor kidney comes with a vein showing an early bifurcation, while there is one large vein on the contralateral side. Management: end to end anastomosis of the short common channel of the donor renal vein with one large vein on the recipient side. (H) Variation 6: while the donor kidney comes with a single renal vein with an early bifurcation, there is no suitable recipient vessel on the contralateral side. Management: end to side anastomosis of the short common channel of the donor renal vein to the inferior vena cava. This figure depicts a handful of the more frequent variations and is not statistically comprehensive in terms of all variations possible in German landrace pigs. Abbreviations used: KG-kidney graft; RK-right kidney; IVC-inferior vena cava; AO-aorta Please click here to view a larger version of this figure.
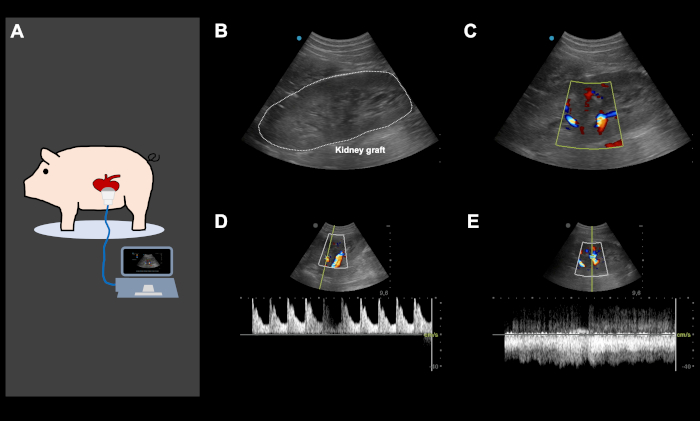
Figure 4: Representative color Doppler ultrasound images, directly after orthotopic kidney auto-transplantation and abdominal closure. (A) Color Doppler ultrasound is performed directly following the implantation of the kidney and abdominal closure, to ensure good arterial and venous perfusion of the kidney graft and to screen for potential iatrogenic vascular kinking. Ultrasound was also used daily and on-demand, based on the clinical performance of the animal to screen for various problems. (B-E) Representative ultrasound images of a kidney graft following implantation. The image of the kidney graft with and without color Doppler (B,C) shows an excellent arterial (D) and venous perfusion (E). This figure show representative images from the same animal. Please click here to view a larger version of this figure.
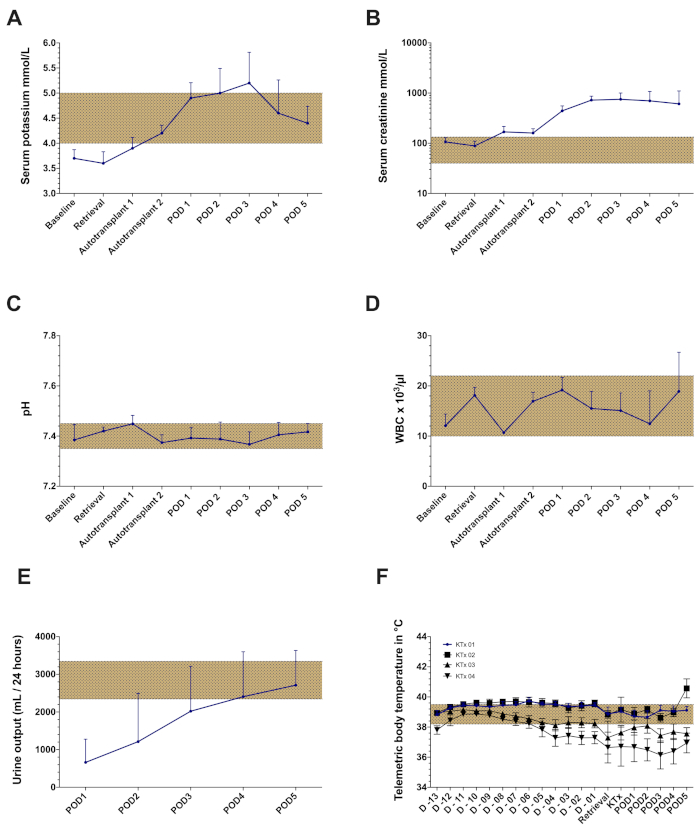
Figure 5: Representative laboratory findings and telemetry data of the orthotopic kidney auto-transplantation model with a cold ischemia time of 24 h. (A) Serum potassium values (B) Serum creatinine values (C) pH (D) White blood cell count (WBC) (E) Urine output. (F) Mean body temperature registered by telemetric monitoring throughout the observation period in four consecutive kidney transplantation (no data presented from the 5th animal due to partial transponder dysfunction). Abbreviations used: POD-postoperative day. Please click here to view a larger version of this figure.
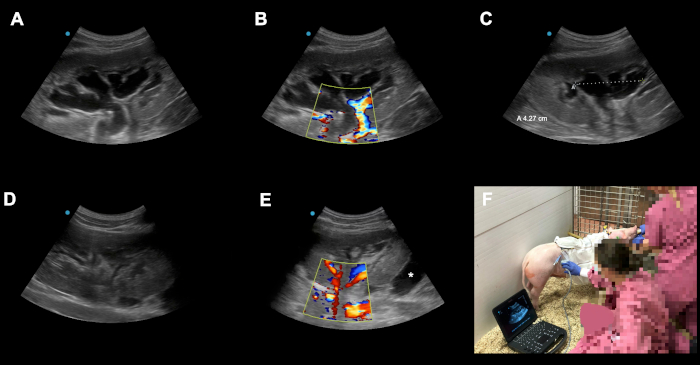
Figure 6: Examples of possible peri-operative complications and pitfalls. (A-C) Postoperative congestion of the transplanted kidney graft on POD3 following orthotopic kindey auto-transplantation. (D) The reason for the congestion was identified as catheter kinking due to an overtightened suture on the level of the skin. After readjusting the suture the congestion resolved almost completely in 24 h. (E) Here an other kidney graft on POD2 following orthotopic kidney auto-transplantation is shown. Asterix (*) shows a fluid collection around the underpole of the graft (bloody collection vs. lymphocele). Because of our technique with closure of the peritoneum over the kidney these collections are usually self limiting due to the advantageous effects of local compression. Animals should be monitored closely in terms of the local finding, signs of bleeding or infection. (F) Qualified color Doppler ultrasound performed daily (and on demand) in the housing facility has, besides its academic utilization (e.g., documentation, registration of arterial resistence indices), a crucial diagnostic role in recognizing potential complications in the early subclinical phase. Please click here to view a larger version of this figure.
| Experimental task/step | Days | Time (min) | Surgeon | Veterinary officer | Veterinary technician | Laboratory technician | Doctoral student | Total |
| Nr | ||||||||
| Preopreative care | D-29 to D-15 | n.a. | 1 | 1 | 1 | 3 | ||
| Telemetry implantation surgery | D-15 | 85±5 | 1 | 1 | 1 | 1 | 1 | 5 |
| Postoperative care following telemetry implantation | D-15 to D-1 | n.a. | 1 | 1 | 1 | 3 | ||
| Graft retrieval surgery | D-1 | 135±32 | 1 | 2 | 1 | 2 | 2 | 8 |
| Kidney auto-transplantation surgery | D 0 | 168 ±27 | 1 | 2 | 1 | 2 | 2 | 8 |
| Postoperative care following kidney auto-transplantation | D 0 to D5 | n.a. | 2 | 1 | 2 | 5 | ||
| Sacrifice | D 5 | n.a. | 2 | 1 | 1 | 4 |
Table 1. Description of the required human resources and time-schedules for performing various experimental steps of the porcine kidney auto-transplantation model.
