To compare the transplant efficacy of fat-covered islet transplantation to that after intraperitoneal islet transplantation, the same number of islets was implanted onto the peritoneum at the left paracolic space of control recipient diabetic animals. The blood glucose levels of mice with fat-covered islet transplantation were observed to gradually and significantly decrease compared to intraperitoneal islet transplanted mice (p = 0.0023; Figure 3A). One month after transplantation, the blood glucose in mice with fat-covered islet transplantation was maintained at lower levels than that observed in intraperitoneal islet transplanted mice as assessed by intraperitoneal glucose tolerance testing (p = 0.0046; Figure 3B). Furthermore, as we have previously, reported that plasma insulin levels also improved after fat-covered islet transplantation. Re-elevation of blood glucose levels was also confirmed. These data demonstrate that intraperitoneal fat-covered islet transplantation using 200 IEQs can significantly improve the diabetic conditions of recipient mice.
Histological examination was also performed to assess islet engraftment into the epididymal white adipose tissue. In fat-covered islet transplant recipient animals, hematoxylin-eosin staining reveals the presence of islets within the epididymal white adipose tissue (Figure 3C, top image). In addition, fluorescence-conjugated antibody staining of insulin-positive islets facilitated the detection of von Willebrand factor-positive microvessels within the epididymal white adipose tissue of all of the recipient mice (n = 6; Figure 3C). In contrast, in intraperitoneal islet transplanted mice, no engrafted islets were observed in either the epididymal white adipose tissue or the abdominal wall (data not shown).
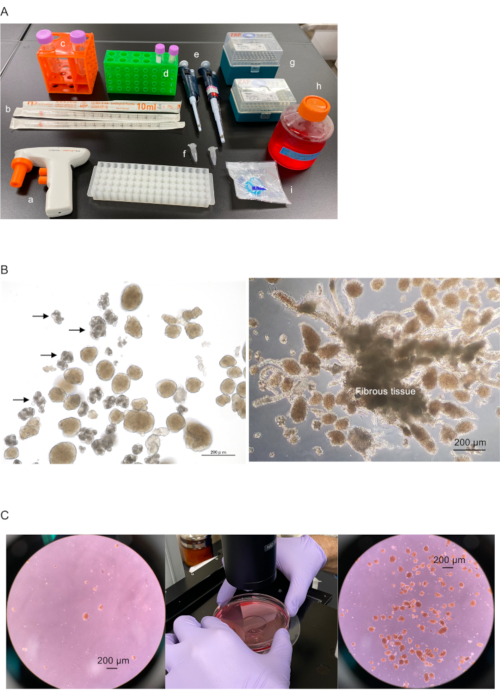
Figure 1-ABC. Preparation of islets for transplantation onto epididymal adipose tissue and covering with epididymal white adipose tissue. (A) Preparation of instruments: a. pipette aid, b. 10 mL pipette tips, c. 50 mL plastic tubes, d. 15 mL plastic tubes, e. 50-200 µL (left) and 200-1000 µL (right) micropipettes, f. 1.5 mL plastic centrifuge tubes, g. 200 and 1000 µL micropipette tips, h. medium or buffer containing albumin or fetal bovine serum (i.e., DMEM with low glucose containing 10% fetal bovine serum and 100 U/mL penicillin + 100 U/mL streptomycin solution), and i. 40 µm cell strainer. (B) Isolated islets with acinar (left: indicated by arrow) and fibrous tissues (right). Scale bar = 200 µm. (C) Collected islets in the plastic tube. Left, dispersed islets in culture dish. Center, islets are collected in the center of the culture dish by swirling. Right, collected islets in center of dish. Scale bar = 200 µm. Please click here to view a larger version of this figure.
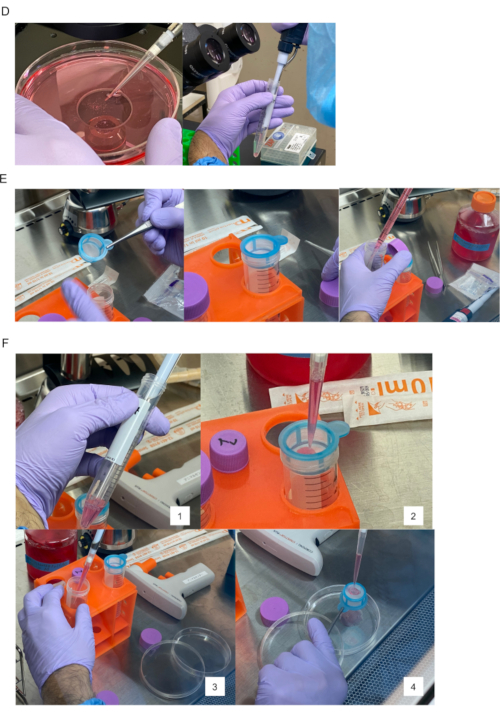
Figure 1-DEF. Preparation of islets for transplantation onto epididymal adipose tissue and covering with epididymal white adipose tissue. (D) Collected islets (left) are transferred into 15 mL plastic tubes (right). (E) The 40 µm cell strainer is set on top of the 50 mL plastic tube (left and center). Prepared medium/buffer added to other 50 mL plastic tube for flushing islets on the cell strainer into a new culture dish (right). (F) 1. Islets collected using a 200-1000 µL micropipette. 2. Islets poured into the cell strainer. 3 and 4. Medium/buffer used to flush islets onto strainer into new culture dish. Please click here to view a larger version of this figure.
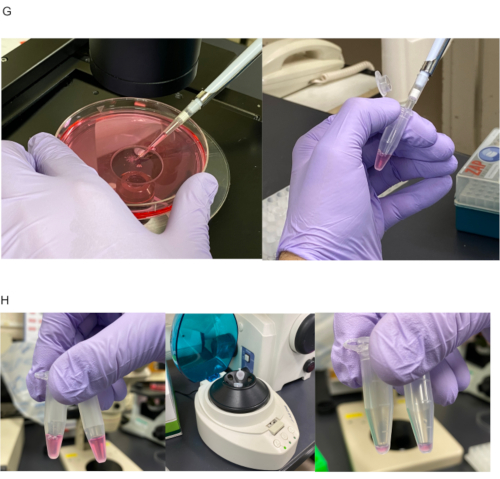
Figure 1-GH. Preparation of islets for transplantation onto epididymal adipose tissue and covering with epididymal white adipose tissue. (G) Islets divided into 1.5 mL plastic centrifuge tube according to number of recipient mice. Here, two hundred 100-200 µm islet equivalent (IEQ) were divided equally into each tube. (H) Islets divided equally in 1.5 mL tubes before centrifugation (left). Islets centrifuged to collect at tube bottom (center). 20-30 µL of supernatant remain in tube after discarding excess solution (right). Please click here to view a larger version of this figure.
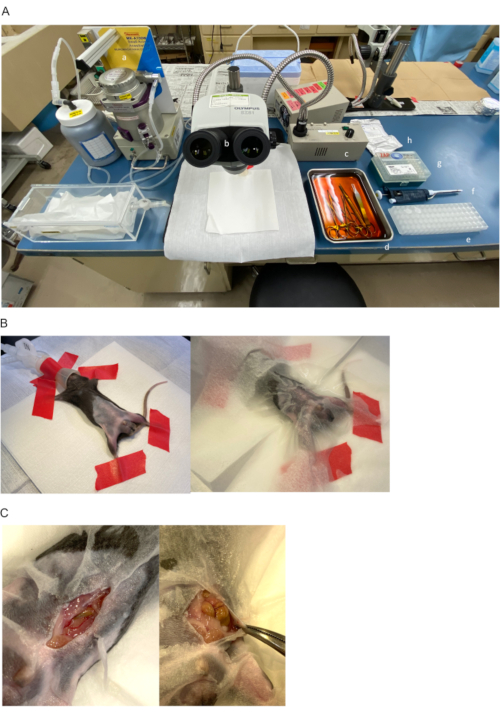
Figure 2-ABC. The procedure of islet transplantation onto epididymal adipose tissue and covering using epididymal white adipose tissue. (A) Preparation of instruments: a. anesthesia machine for small animals, b. stereo microscope, c. light source, d. disinfected surgical instruments, e. divided islets in 1.5 mL plastic tubes, f. 50-200 µL micropipettes, g. 200 µL micropipette tips, and h. 4-0 sutures. (B) Diabetic recipient mouse in a supine position under general anesthesia of 2% isoflurane (left). The abdomen and the inguinal region are disinfected using 70% ethanol and covered by a paper lab wipe (right). (C) Skin is incised at lower median position (left). Left abdominal wall is clamped by Pean forceps and pulled to left side of mouse to secure surgical field (right). Please click here to view a larger version of this figure.
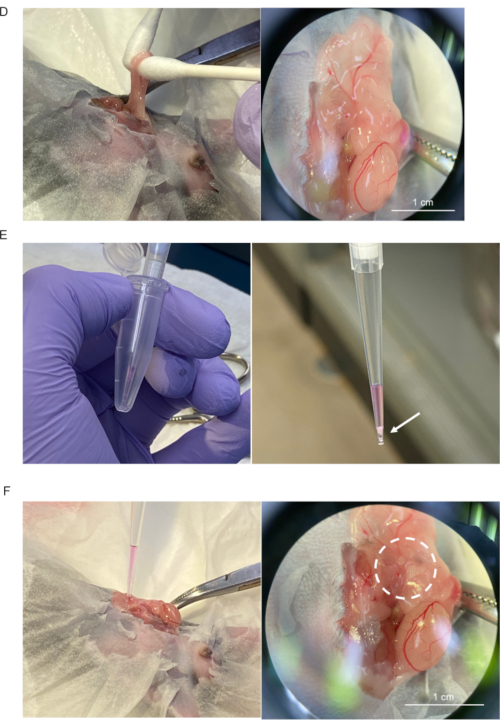
Figure 2-DEF. The procedure of islet transplantation onto epididymal adipose tissue and covering using epididymal white adipose tissue. (D) The left epididymal white adipose tissue and the left testis are mobilized outside of the abdomen (left) and distended (right). Scale bar = 1 cm. (E) Islets in 1.5 mL plastic tubes are completely collected using a micropipette with 200 µL pipette tip (left). Collected islets (indicated by arrow) allowed to completely sink by gravity to pipette tip (right). (F) Micropipette tip lightly placed onto the distended adipose tissue (left). Islet seeding (dotted circle) onto the tissue confirmed by dissecting microscope (right). Scale bar = 1 cm. Please click here to view a larger version of this figure.
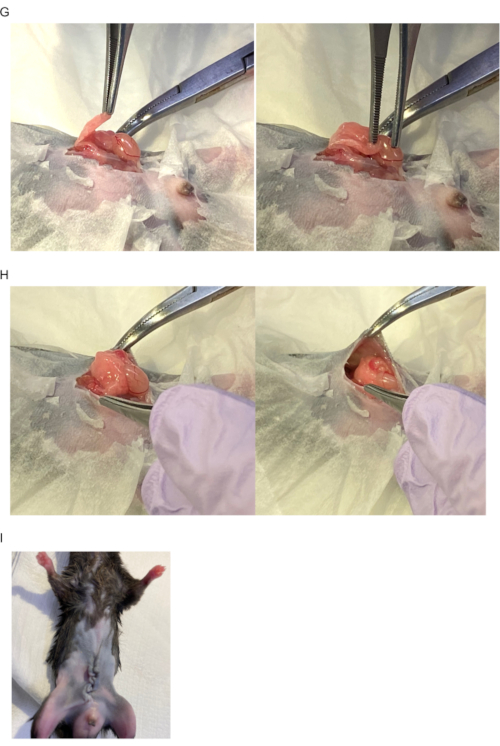
Figure 2-GHI. The procedure of islet transplantation onto epididymal adipose tissue and covering using epididymal white adipose tissue. (G) Islets are covered with epididymal white adipose tissue. (H) Left testis and epididymal white adipose tissue returned to intraperitoneal cavity. (I) Image after abdomen closure. Please click here to view a larger version of this figure.
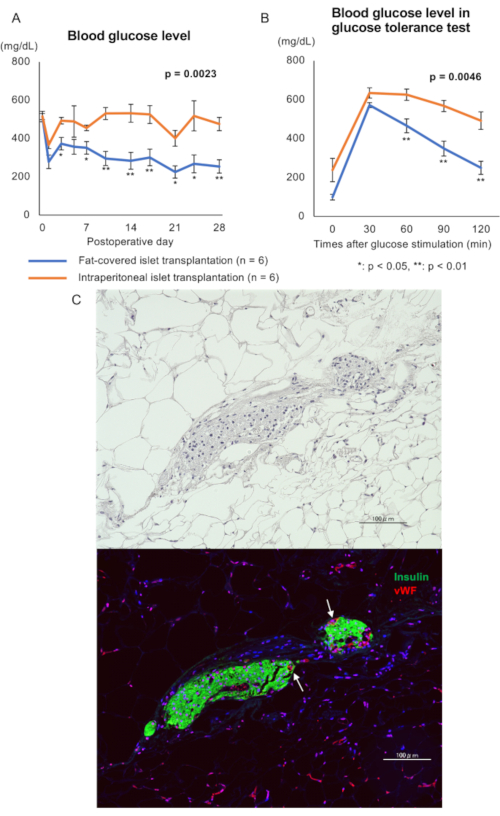
Figure 3. The therapeutic effect of fat-covered islet transplantation. (A) Blood glucose level. Blue line: fat-covered islet transplantation (n = 6); Orange line: intraperitoneal islet transplantation (n = 6) Statistical analysis was performed using repeated measures analysis of variance and a significant difference was defined as p < 0.05. (B) Blood glucose level from glucose tolerance test a month after transplantation. Blue line: fat-covered islet transplantation (n = 6); Orange line: intraperitoneal islet transplantation (n = 6). Statistical analysis was performed using repeated measures analysis of variance and a significant difference was defined as p < 0.05. (C) Histological image of engrafted islets one month after transplantation. Top image: hematoxylin-eosin staining; Bottom image: immunohistostaining for murine insulin (green) and von Willebrand factor (vWF: red, indicated by white arrow). Scale bar = 100 µm. Please click here to view a larger version of this figure.
