Images captured via Optical Coherence Tomography (OCT) are shown for OG injured eyes to illustrate how a successful injury induction looks. Figure 3 shows images for control and OG injured AS tissue immediately after injury and 72 h later. Two views are shown: cross-sectional images through the injury site and top-down maximum intensity projection (MIPs) to visualize the surface area of the image. Control eyes show no noticeable disruption in the cornea, while clear injuries can be located that cross the entire cornea after OG injury. From MIPs, it is evident that injuries are irregular in shape and size, but the injury size does decrease over 72 h. Previously, this effect has shown to be significant for a number of injury sizes tested13.
The primary data output for the OG injury model described in this protocol is intraocular pressure over the course of the experimental setup. Data is recorded in units of millivolts as an output from each pressure transducer which can be converted into mmHg via calibration (Supplementary Protocol 4). Example IOP data vs the experimental time course is provided for eyes that are considered acceptable and others that would not be considered usable (Figure 4A). From the pressure trace data, eyes were attached to sensors after 24 h in culture, but IOP continues to fluctuate over the first 72 h in culture. Physiological IOP for AS tissue in organ culture is approximately 8-10 mmHg, so 2x and ½x range was decided upon as a gate for usable IOP values after values have stabilized (5-20 mmHg). Only eyes that were in that range would be allowable for use with the remainder of the protocol. From prior experiments, we had a 90% success rate that was achieved in ASOC setup for eyes stabilizing in the required range (Figure 4B).
The results for how IOP changes due to OG injury and therapeutic intervention are also provided (Figure 4C,D). After OG injury induction, pressure should significantly drop and remain that way until the tissue is removed from ASOC (Figure 4C). If an eye after injury induction does not decrease in pressure, this indicates that a successful injury was not induced as IOP should be reduced if the watertight seal of the eye is compromised. However, smaller injury sizes may self-heal, which could result in IOP being restored. If therapeutic is applied to the eye after OG injury induction, restoration of IOP can be tracked during ASOC. This concept is demonstrated with data showing a Dermabond adhesive applied to 2.4 mm OG injuries (Figure 4D). Average results for five separate ASOC experiments with and without therapeutic are shown and it is evident the therapeutic is increasing IOP. This method can measure the efficacy of the therapeutic for restoring IOP and track whether that pressure is restored across the key 72 h post-OG injury.
Further, the ASOC protocol is adaptable for use with a wide range of characterization endpoints to meet the end user's experimental requirements. During culture, outflow media leaving the eye can be collected on a daily or even hourly basis which can be utilized for tracking protein level changes occurring during ASOC, after OG injury induction, or after therapeutic is applied. For instance, gelatin zymography has been previously performed to detect matrix metalloproteinase levels to track wound healing and tissue remodeling20. Further biological endpoints are possible after removing tissue from culture via traditional immunohistochemistry methods for assessing tissue viability21,22, tracking pathophysiological changes to the cornea23,24, or antibody-based staining for any protein of interest25,26.
Functional corneal metrics can also be obtained from eyes maintained in ASOC. Corneal epithelium integrity can be assessed via a fluorescein eye stain and image acquisition using a blue light source27,28. After removal from culture, corneal tissue can be assessed for transparency through simple image acquisition13. Traditional ocular imaging can also be performed to assess tissue structure with or without therapeutic intervention. OCT images, as shown in Figure 3, can create cross sectional images through the cornea and can be captured non-invasively, potentially allowing image collection while maintaining tissue in culture. Other imaging modalities such as slit-lamp microscopy, ultrasound, or in vivo confocal microscopy can also be adapted for acquiring further anatomical information.
Lastly, assessment of mechanical properties of the anterior segment can be captured to understand the effect of the OG injury or subsequent therapeutic on the underlying tissue. While IOP data collection alone highlights how the integrity of the watertight seal of the eye has been compromised, we have previously shown that additional test metrics can be measured to tease out additional mechanical features10,11. Ocular compliance, a lumped mechanical property describing how intraocular pressure changes due to inflation (change in volume/change in pressure), can be measured with a syringe pump to inject sudden small volumes of fluid into the eye and recording the resulting pressure increase with a pressure transducer. Higher compliance indicates the tissue is less stiff and can be used to track how therapeutic material properties differ from the underlying corneal tissue. Leak rate from the eye or a traditional outflow facility can be measured and calculated to determine the precise fluidic flow rate leaving the eye per unit of pressure20,29. Lastly, with regards to therapeutic testing, burst pressure can be measured to determine the maximum pressure the eye can hold prior to the therapeutic failing. This can be used to compare performance to uninjured eyes or to track changes in performance with time12,13.
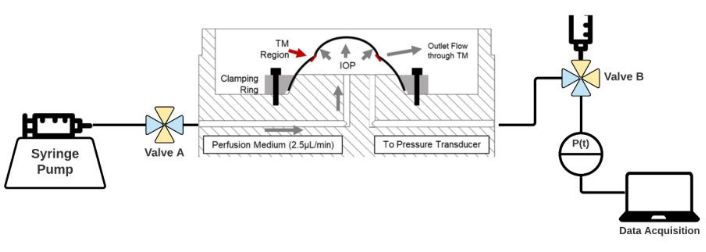
Figure 1: Diagram of the ASOC setup. Eyes are held in custom-built organ culture dishes and held in place with a clamping ring. ASOC media is infused via syringe pump through Valve A and connected to a pressure transducer, and subsequent data acquisition with Valve B. Open ports in each valve are highlighted in blue while yellow indicates closed channels. Please click here to view a larger version of this figure.
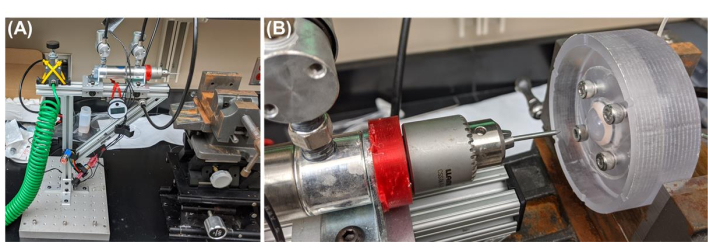
Figure 2: Overview of the OG injury setup. (A) Pneumatic powered injury device setup. From left to right, compressed air is introduced to the device via a compressed air line, which passes through a regulator to set pressure at 50 psi as measured by the pressure gauge. Two solenoid valves are connected to a linear actuator to direct expansion/retraction of the drill chuck holding the puncture object. Vise is positioned in front of the puncture device to hold the eye at the appropriate x, y, z positioning. (B) Representative ASOC is placed in front of the injury induction device. Further details of the device and its construction are detailed in Supplementary Protocol 3. Please click here to view a larger version of this figure.
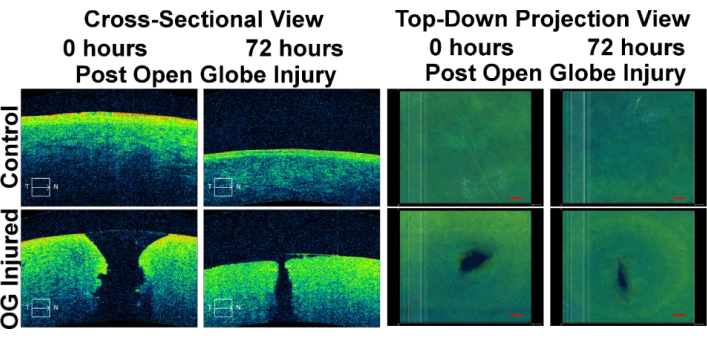
Figure 3: Optical Coherence Tomography Images of ASOC OG injury experiments. Images are shown for control eyes (uninjured) and OG injured eyes immediately post-injury and 72 h post-injury. Views are shown as cross-sections through the cornea (left side) and top-down maximum intensity projection views of the corneal surface (right side). The figure has been adapted with permission from Snider et al.13. Please click here to view a larger version of this figure.
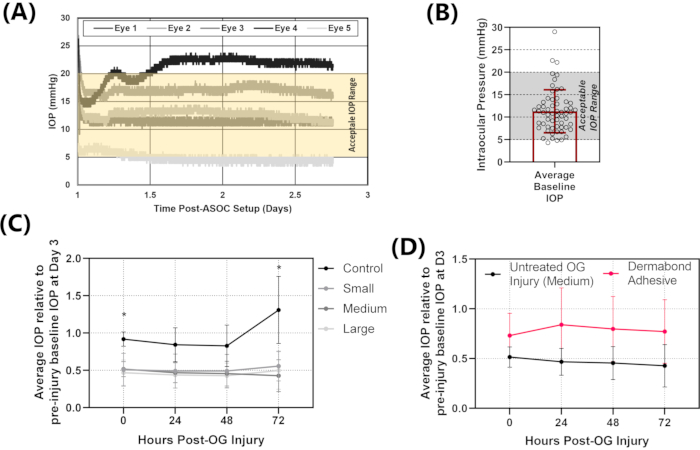
Figure 4: Representative IOP results for ASOC experiments. (A) Raw IOP data for the first 72 h of ASOC setup. Eyes are punctured at 72 h so the first 3 days of data are assessed to determine whether IOP stabilizes in the acceptable IOP range (5-20 mmHg). From the representative results, three of the five eyes fall within the acceptable IOP range, while one has IOP too high and one has IOP too low (falling outside of the highlighted yellow region on the plot). (B) Stabilized IOP for n = 50 ASOC setups from previous experiments to demonstrate the typical success rate with the ASOC method. (C) IOP for uninjured eyes compared to three different OG injury sizes after injury induction for 72 h. The loss of IOP is evident, with no signs of recovery. (D) Injured IOP results compared to injuries treated with a Dermabond adhesive. While the error rate is high due to some eyes being sealed and others not, the method can track changes to IOP over the 72 h period post-injury. The figure has been adapted with permission from Snider et al.13. Please click here to view a larger version of this figure.
Supplemental Files. Please click here to download these files.
