System calibration
The data analysis software allows for direct calibration of a custom flowhead, such as the one described herein. This is performed when setting the Spirometry Flow. As described in step 3.1, an option exists to input the known calibration air volume, which calculates the voltage to volume correlation coefficient within the system. This, however, generates a correlation coefficient based on a single read, and it has been observed that the inherent variation of calibration from an n = 1 standard has poor utility. The current approach can address this shortcoming and allows a user to perform a daily calibration using multiple readings averaged to calculate a calibration coefficient. Calibration with 20 µL of injected air was demonstrated herein, representing a typical high-end breath volume in a typical mouse. The software assumes an origin intercept (0,0) and is thus calibrated from 0-20 µL using this approach.
The methodology proposed here for sWBP calibrates daily, thus accounting for any fluctuations in environmental humidity/temperature. The original methods used for specific WBP, date back to the methodology of Drorbaugh and Fenn from 1955, who developed WBP for measuring ventilation in human infants5. The Drorbaugh and Fenn calculations account for variations in temperature and humidity of the environment and the subject. The current approach corrects for environmental fluctuations by calibrating each sWBP session. Still, it was decided to address whether the heating and humidification of breathing across the nasal cavity/lung of a mouse affect the measurement of a known volume of air. Thus, an artificial apparatus was created to mimic the subject's effect on heating and humidifying calibrated air measurements. Luer connectors were attached to a 15 mL conical tube and placed this sealed conical in-line between the sample chamber and the gas-tight calibration syringe. A 20 µL calibration was performed using an empty conical tube held at room temperature (23 °C). The conical tube was then partially filled with distilled water to just below the Luer connectors, allowing time to equilibrate the headspace of the conical; the calibration volume was then re-measured to investigate the effect of humidity. The conical tube was placed in a heating block and equilibrated at 37 °C in a humid environment, and finally equilibrated to 37 °C with no water to assess the effect of subject heating and with no additional contribution of humidity. Figure 2 demonstrates that all conditions tested did not significantly impact the calibrated 20 µL measurement delivered by the gas-tight syringe. From this finding, it was concluded that sWBP offers an accessible approach to monitor breathing in research animals without the need for complex calculations predicated on the temperature and humidity of the animal subject, as these make no significant impact on measured breath volume.
Subject monitoring
sWBP was used to monitor breathing during the disease of lethal respiratory infections with the bacterial pathogen B. pseudomallei. One challenge of monitoring breathing in conscious animals is the curiosity of normal healthy animals moving within the sample chamber. The movement of the mouse creates a constantly moving baseline that can be mitigated in part by pre-conditioning subjects to the chamber over a period of several days prior to measurement. This issue primarily affects the baseline measurement in healthy mice, as the subjects become lethargic during infection, making sWBP much more manageable with reduced subject activity. It may be tempting to attempt to use some form of restraint, whether physical or anesthesia. The use of physical restraint may affect natural breathing by causing stress. Further, the use of anesthetics is known to have pronounced effects on breath rate and depth10; thus, it was decided to investigate the impact of anesthesia with the in-house sWBP apparatus. Isoflurane is commonly used to perform in vivo diagnostic imaging during the infection models, and therefore, a C57BL/6 mouse was anesthetized and monitored progression until recovery out of anesthesia using sWBP. This trial was conducted with a juvenile 4-week old albino C57BL/6J mouse to prolong the window of recovery from anesthesia. Figure 3 demonstrates that the preferred anesthetic causes mice to exhibit a slow breath rate with a large tidal volume of air. As mice begin to recover from sedation, their breath rate increases and breath volume decreases, with the net effect that total inspired air slowly increases. In this trial, it was found that the breath volume is restored to pre-anesthesia levels within the first 30 s of recovery. The breath rate steadily increases until the baseline breathing is restored to 2-2.5 min post-removal from anesthesia. The minute volume closely followed the effects of breath rate, reaching baseline minute volume by 2.5 min post-removal from anesthesia. This finding supports that anesthesia should not be employed in the sWBP approach. It dramatically affects baseline breathing, not surprisingly, as anesthesia will slow the host metabolism, creating a reduced demand for inspired oxygen. Sanitation of the sample chamber should also be considered between subjects to address study-specific infection control as well as the impact of pheromones from urine or feces which could impact the stress between subjects.
WBP is an attractive strategy for monitoring lung function in respiratory disease models in a non-invasive manner. sWBP was used to study how breathing changes during lethal respiratory melioidosis infections (Figure 4), with time points mirroring bioluminescence monitoring in the lung. It was observed that this model is associated with an early onset of lethargy, which persists in a slowly progressive manner until the development of the moribund disease at approximately 3 days post-infection. It was also observed that the breath rate and total inspired air (minute volume) of the mice decrease rapidly during the first day of infection and remain low for the remainder of the course of infection (Figure 4A,C). This pattern is consistent with the early onset lethargy, which persists for the next 2 days of the infection. In contrast, the breath volume does not steeply drop during the first 24 h and instead has a slight and steady decrease, which approaches a linear decline over the 3-day course of the disease (Figure 4B).
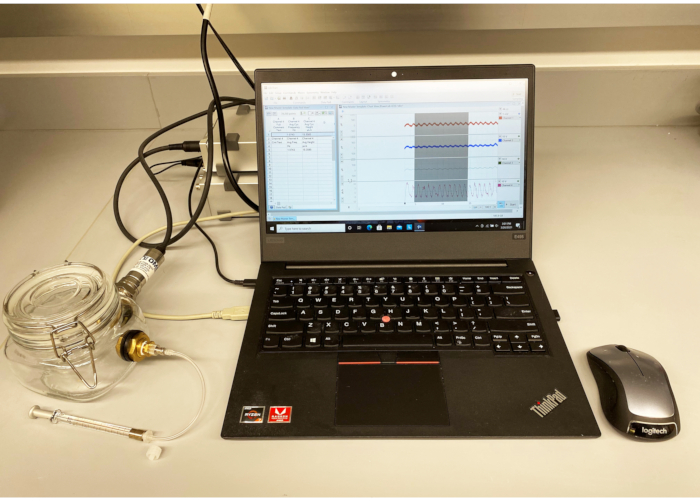
Figure 1: sWBP apparatus. A custom Sample Chamber was constructed from a sealable square glass jar with bulkhead connectors on two flat faces. One bulkhead was used to mount a gauge pressure sensor connected to a bridge amplifier and data acquisition device digitizer via an 8-pin DIN connection. The second bulkhead was fitted with a Luer connector for calibration by a gas-tight syringe. The device was connected to a PC running the software. Please click here to view a larger version of this figure.
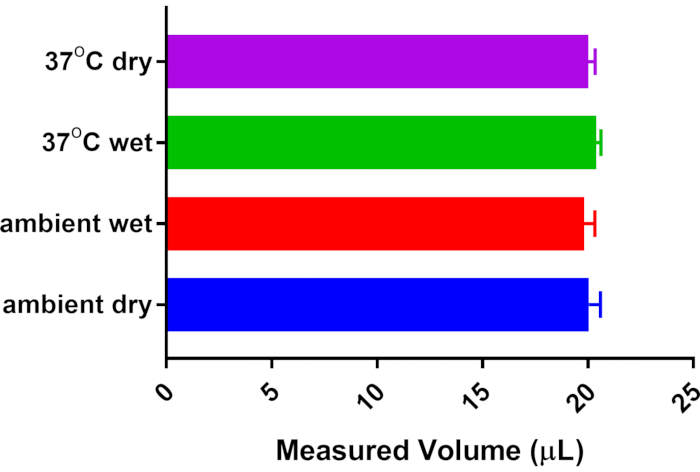
Figure 2: Effect of subject temperature and humidity on breath volume. A 15 mL conical tube with Luer connectors was installed in-line between the 20 µL calibration syringe and the Sample Chamber. The system was calibrated to 20 µL with no additional temperature/humidity contribution from the conical tube. Other measurements were collected post-equilibration with saturated humidity from distilled water and/or warming of the conical tube from room temperature (23 °C) to body temperature (37 °C). No significant difference was detected from n = 5 measurements of each condition by One-way ANOVA with Tukey's Multiple Comparison post-test. Please click here to view a larger version of this figure.
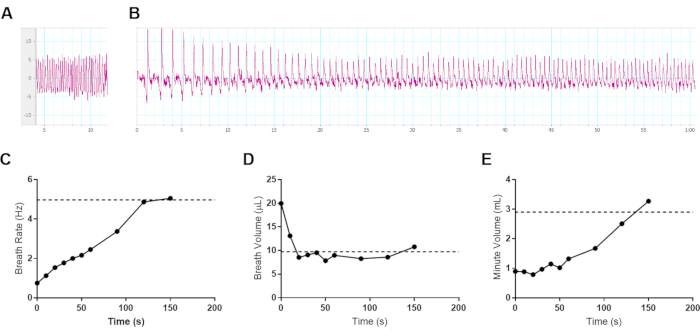
Figure 3: Effect of gas anesthesia on breathing in mice. Representative data from a 4-week old female albino C57BL/6J mouse (8.6 g) was sedated for 5 min with 3% isoflurane in oxygen and transferred to an sWBP Sample Chamber. Pleth data was collected for 150 s following removal from anesthesia. The subject began initial ambulation by 100 s following removal from anesthesia. (A) Baseline breathing before anesthesia, measuring a 4.97 Hz breath rate, 9.74 µL breath volume, and 2.91 mL minute volume. (B) The first 60 s of changes to breathing during recovery from anesthesia. (A–B) Vertical axis measuring µL per breath and horizontal axis in seconds. (C–E) Ventilation data was collected during the 150 s of recovery from anesthesia, averaged from ≥3 breath cycles per time point for (C) Breath Rate, (D) Breath Volume, and the (E) calculated Minute Volume. The pre-anesthesia baseline values are indicated with a horizontal dotted line in each respective graph. Please click here to view a larger version of this figure.
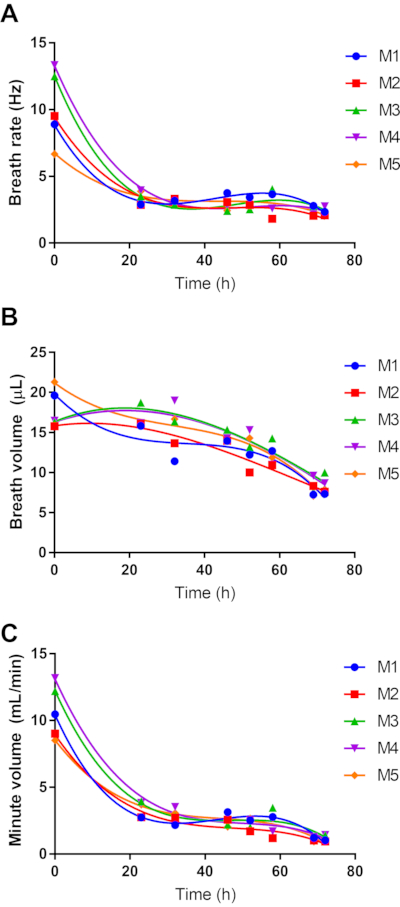
Figure 4: Effect of respiratory melioidosis on host breathing. Five 8-week female C57BL/6 mice were infected with 4.9 log CFU of bioluminescent B. pseudomallei strain JW270. sWBP was conducted throughout the 3-day course of infection, measuring Breath Rate (A) and Breath Volume (B). The total inspired air was calculated as the Minute Volume (C). Data for each of the five subjects are independently plotted with third-order polynomial regression. Please click here to view a larger version of this figure.
