Measurements of Cilia Beat Frequency (CBF) and pattern have been established as diagnostic tools for respiratory diseases such as Primary Ciliary Dyskinesia (PCD)1. In Cystic Fibrosis (CF), dysfunction of the CF Transmembrane conductance Regulator (CFTR) chloride channel causes dehydration of the airway surface liquid and impaired mucociliary clearance2. Ciliary function has been investigated in vitro in primary airway cell models as an indicator of CFTR channel activity3. However, considerable patient-to-patient variability exists in CBF in response to CFTR-modulating drugs, even for patients with the same CFTR mutations3. Furthermore, the impact of dysfunctional CFTR-regulated chloride secretion on ciliary function is poorly understood. There is currently no comprehensive protocol demonstrating sample preparation of in vitro airway models, image acquisition, and analysis of CBF.
Nasal epithelial sheets isolated from nasal mucosal brushings are directly used for measurements of ciliary function for PCD diagnosis4. Yet, while there is no control over the size or quality of the nasal epithelial sheets obtained, CBF varies depending on whether it is measured on single cells or cell sheets and on epithelial sheet ciliated edges that are disrupted or undisrupted5. As such, secondary dyskinesias caused by damage to cells during the collection of nasal mucosal brushings may influence CBF. Primary cell culture of nasal epithelial cells and their differentiation at Air-Liquid Interface (ALI) or in three-dimensional basement membrane matrix into ciliated airway epithelial organoids give rise to cilia that are free from secondary dyskinesias4,6,7,8. Airway epithelial cells differentiated at ALI (henceforth termed ALI models) have been deemed an important secondary diagnostic aid that replicate the ciliary beat patterns and frequency of ex vivo nasal mucosal brushings6 and enable analysis of ciliary ultrastructure, beat pattern, and beat frequency while retaining patient-specific defects9. Yet, discrepancies exist in the methodologies used to create these pseudostratified, mucociliary differentiated cell models. Different culture expansion or differentiation protocols could induce distinct epithelial phenotypes (ciliated or secretory)10 and result in significant differences in CBF11. CBF has been quantified in nasal epithelial brushings4,6,12,13,14,15,16, airway epithelial organoids14,17,18 and ALI models3,4,6,13,19,20,21. Yet, amongst these protocols, there are large variabilities, and often many parameters are not controlled for. For example, in some studies, CBF is imaged in situ while the cells of the ALI model remain on the permeable support insert3,19,20,21, yet others scrape the cells from the permeable support insert and image them suspended in media4,6,13.
Furthermore, the wider application of techniques that measure ciliary function is limited by the extreme susceptibility of ciliary function to changes in environmental factors. Environmental factors such as temperature22, humidity23,24, and pH25,26 influence ciliary function and must be regulated to quantify CBF accurately. The various physiological parameters used across different laboratories and how they influence CBF has been reviewed previously27.
Various imaging technologies and approaches to CBF measurements are reported in the literature. For PCD diagnostics, video microscopy is used to measure ciliary function28,29. Recently, a video analysis algorithm based on differential dynamic microscopy was used to quantify both CBF and cilia coordination in airway epithelial cell ALI models3,30. This method enables the characterization of ciliary beating in airway epithelial cells in a fast and fully automated manner, without the need to segment or select regions. Various methods for imaging and quantification of CBF may add to the differences reported in CBF in the literature (Supplementary File 1).
A protocol from culture to quantification to streamline existing methods, standardization of culture conditions, and image acquisition, performed in strict environmentally controlled conditions, would enable consistent, reproducible quantification of CBF within and between individuals.
This protocol provides a complete description of the collection of epithelial cells, expansion and differentiation culture conditions, and quantification of CBF in three different airway epithelial cell model systems of nasal origin: 1) native epithelial sheets, 2) ALI models imaged on permeable support inserts and 3) Extracellular Matrix (ECM)-embedded three-dimensional organoids (Figure 1). Nasal epithelial cells obtained from nasal inferior turbinate brushings are used as representatives of the airway epithelium since they are an effective surrogate for bronchial epithelial cells31 while overcoming the invasive procedure associated with collecting bronchial brushings. The Conditional Reprogramming Cell (CRC) method is used to expand primary airway epithelial cells for the creation of ALI models and three-dimensional organoids. Conditional reprogramming of airway epithelial cells to a stem cell-like state is induced by co-culture with growth-arrested fibroblast feeder cell system and Rho-associated kinase (ROCK) inhibitor32. Importantly, the CRC method increases population doubling in airway epithelial cells while retaining their tissue-specific differentiation potential33,34. In all airway epithelial cell models, the ciliary function is captured in a temperature-controlled chamber using a high-speed video camera with standardized image acquisition settings. Custom-built scripts are employed for the quantification of CBF.
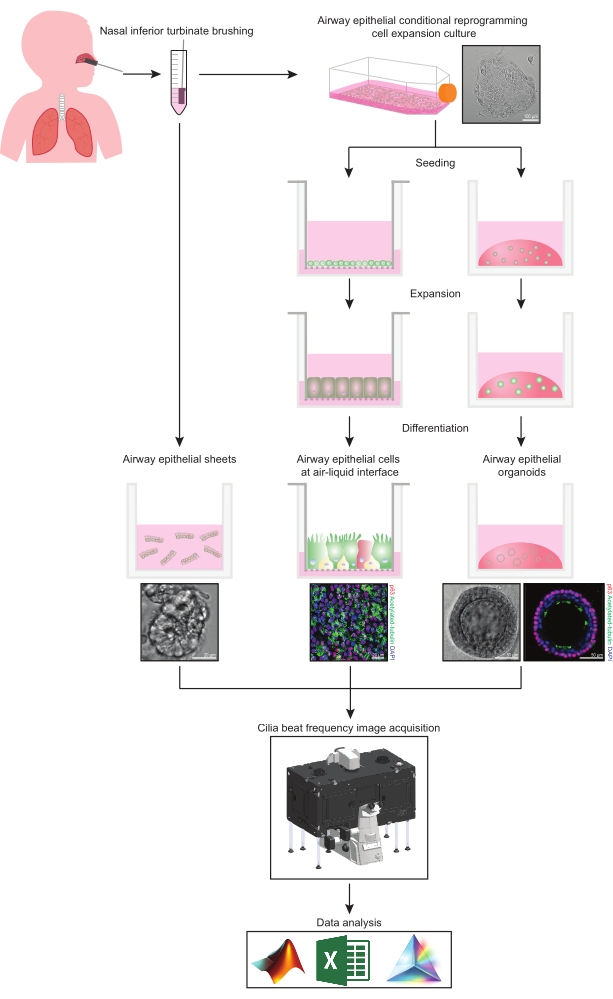
Figure 1: Schematic of workflow. Following brushing the participants' nasal inferior turbinate, airway epithelial cells are utilized in one of two ways. Either airway epithelial sheets are isolated, and cilia beat frequency is imaged immediately, or airway epithelial cells are expanded via the conditional reprogramming cell method. CRC-expanded airway epithelial cells are differentiated to establish airway epithelial cells at an air-liquid interface or airway epithelial organoid cultures. Imaging of ciliary beat frequency is acquired using a live-cell imaging microscope with a heating and humidity environmental chamber and a fast frame rate (>100Hz) scientific camera. Data analysis is performed using custom-built scripts. Please click here to view a larger version of this figure.
