In a proof-of-concept study, 22 adult male Wistar rats (200-400 g) were randomly assigned into two groups: STIM (n = 15) and SHAM (n = 7). All animals were housed individually in polycarbonate cages, in a climate-controlled room (21-22 °C), having free access to water and dry food throughout the study. The transesophageal stimulation protocol described above was applied to all animals for 10 days, 5 days per week. All animals underwent the same protocol, except that the rats in the SHAM group did not receive active electrical stimulation.
As expected, no episodes of AF were induced in the SHAM animals throughout the protocol. Hence, no other parameters (i.e., the duration of AF episodes and the presence of 'persistent' AF episodes) could be evaluated in this group.
On the first day of stimulation, 12 (80%) of the 15 STIM animals presented AF episodes (Relative Risk = 3.33, p < 0.001 vs. the SHAM group using Fisher's exact test). In the STIM rats, out of 164 stimulation cycles applied on the first day of stimulation, 42 were followed by AF episodes (median inducibility of 20% [interquartile range of 6.67-72.22] vs. 0% in the SHAM group) (Figure 5).
During the 10 days of protocol, AF was efficiently induced in all animals (Figure 6). An average of 15.6 ± 8.7 episodes of AF was induced in the STIM animals during the entire duration of the protocol. Of the total number of stimulation cycles applied, 20.05% were followed by AF, and 41 (17.30%) episodes of AF lasted more than 600 s. The average duration of AF episodes lasting less than 600 s is 40.12 s (Table 1).
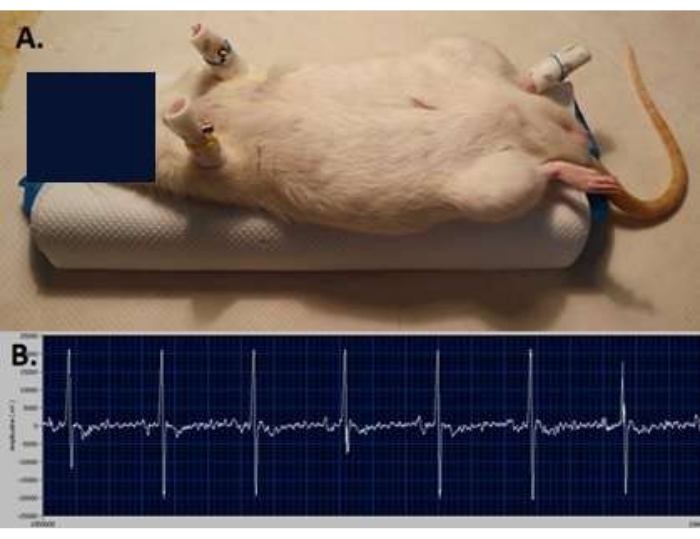
Figure 1: Surface ECG recording. (A) ECG electrodes positioning—two at the level of the forelimbs and one on the left hindlimb of the animal. (B) Surface ECG tracing recorded before applying electrical stimulation. Please click here to view a larger version of this figure.
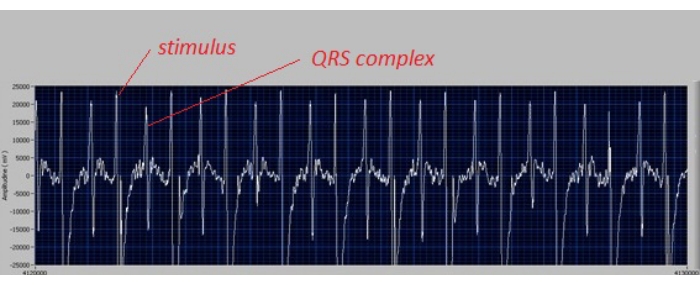
Figure 2: ECG tracing confirming capture of the atria. The ECG tracing confirms the correct position of the catheter, i.e., a narrow QRS complex is observed after each electrical stimulus at a frequency of 400 stimuli/minute. Please click here to view a larger version of this figure.
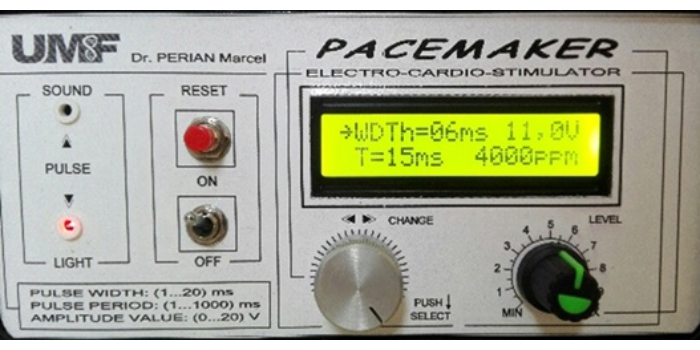
Figure 3: Microcontroller-based cardiac pacemaker settings. Stimulation parameters are set at a frequency of 4,000 stimuli/minute (ppm: pulses per minute), stimulus duration of 6 ms (WDTh: width), and tension of 11 V (i.e., 3 V above the diastolic threshold). Please click here to view a larger version of this figure.
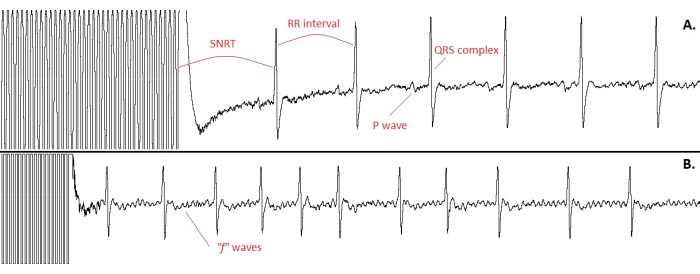
Figure 4: ECG tracings confirming the effectiveness of the stimulation protocol. (A) The sinus node recovery time (SNRT). Note that the time interval at the cessation of stimulation (SNRT) is longer than the cycle length recorded during sinus rhythm (RR interval, i.e., the interval between the R-waves of two consecutive QRS complexes, representing the duration of a cardiac cycle). (B) The appearance of an atrial fibrillation episode after completion of the atrial electrical stimulation cycle. Note the irregular, narrow QRS complexes, the absence of P waves, and the small, distorted "f" waves. Please click here to view a larger version of this figure.
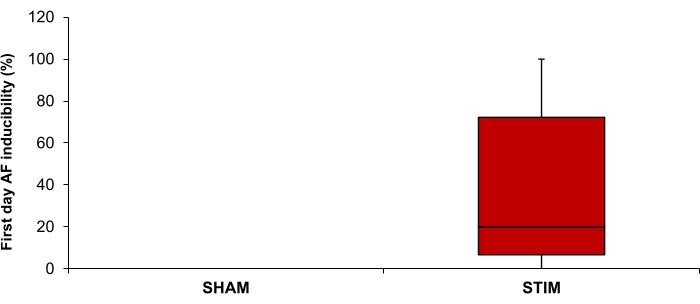
Figure 5: Inducibility of atrial fibrillation (AF) on the first day of stimulation in the STIM (n = 15) and SHAM (n = 7) groups. Data are expressed as median and interquartile range. Please click here to view a larger version of this figure.
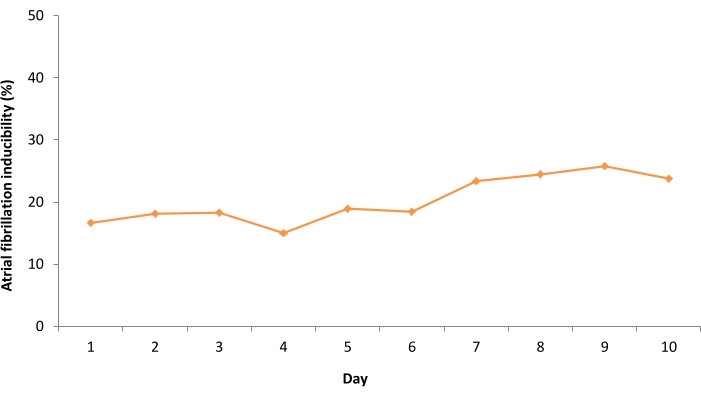
Figure 6: Mean daily inducibility of atrial fibrillation during the 10 days of the stimulation protocol in the STIM rats. Please click here to view a larger version of this figure.
| Electrically-induced atrial fibrillation episodes (n = 237) | Number (%) | Mean duration (seconds) |
| duration ≥600 seconds | 41 (17.30%) | – |
| duration < 600 seconds | 196 (82.70%) | 40.12 |
Table 1: Temporal parameters of electrically-induced 'persistent' and 'non-persistent' atrial fibrillation episodes in the STIM group.
