This protocol has been generated for a prospective clinical trial and co-clinical research. The study was compliant with the Health Insurance Portability and Accountability Act (HIPAA) and approved by the Stanford University institutional review board (IRB). All patients or their legally authorized representative signed a written informed consent, and all children between 7 and 18 years of age signed an assent form.
1. Installing and starting the T2 Fit Map plugin
- Start the Osirix software. Install the T2 Fit Map plugin from the plugin manager and restart the software.
- On the menu bar, click the Plugins button. Click on the drop-down menu and select Install a plugin package (Figure 1).
- Once the plugin manager is loaded, select the available plugins from the drop-down menu and then T2 Fit Map (Figure 2).
- Click download & install. Close the plugin manager and restart the software.
- Load the multi-echo gradient echo sequence images as DICOM files into the software.
- Change the mouse button function to draw a Region of Interest (ROI) (Figure 3).
- Using this mouse button function, define a shape for the required ROI: select Oval or Closed Polygon, or the desired shape from the drop-down menu (Figure 4).
- Draw ROIs in the required images with different echo times (TEs).
- Select the ROIs in all the images with different TEs for which the T2* map is required.
- Click the Plugins button, select Image filters from the drop-down menu, and then select T2 Fit Map.
- Click on T2 Fit Map. A dialog box will open; click on Generate Map (which is located at the bottom of the dialog box) (Figure 5).
NOTE: A fitting curve is generated with minimum, mean, and maximum T2* values for the selected ROIs with various TEs (ms). The mean T2* value is calculated and displayed below the curve (Figure 6).
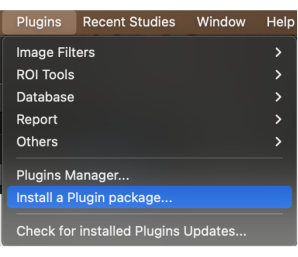
Figure 1: Selecting 'Install a plugin package' from the drop-down menu. Please click here to view a larger version of this figure.
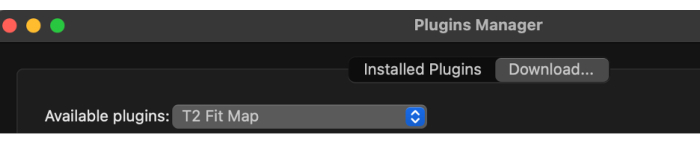
Figure 2: Selecting 'T2 Fit Map' from the available plugins. Please click here to view a larger version of this figure.
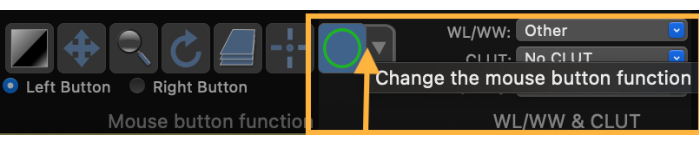
Figure 3: Screenshot demonstrating how to change the mouse button function to draw a region of interest (ROI). Please click here to view a larger version of this figure.
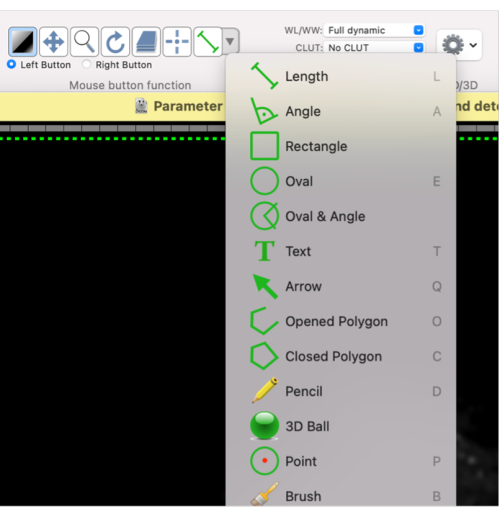
Figure 4: Screenshot showing how to select different shapes for the ROI. Please click here to view a larger version of this figure.
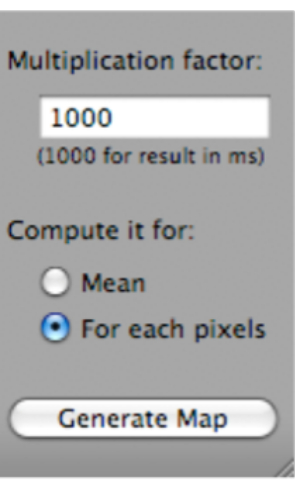
Figure 5: Screenshot showing how to select 'Generate Map' after selecting 'T2 Fit Map'. Please click here to view a larger version of this figure.
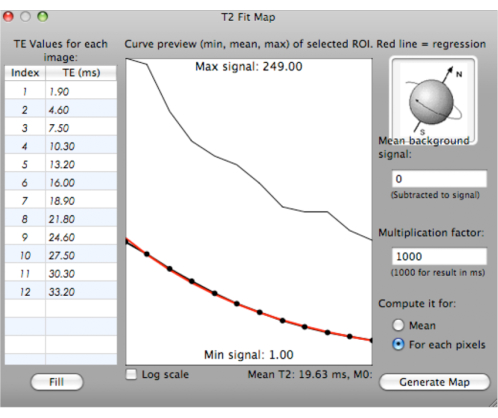
Figure 6: Screenshot showing the generation of a fitting curve for T2* values. Please click here to view a larger version of this figure.
2. Exclusion of noise using the definition of mask
NOTE: To define a mask on the first echo of the T2map_MSME data used to calculate the parametric maps, set a lower first-echo signal threshold for T2* value calculation (the T2* map volume will now exclude the pixels with signals too low for accurate calculation at the first multi-spin multi-echo (MSME) echo. The threshold can be increased to exclude more pixels, or decreased to include more pixels).
- To define the mask ROI on an image series outside the parametric data, open the desired series (e.g., first echo of the T2map_MSME with TE = 15) and select a slice.
- At bottom of the ROI drop-down menu, select Grow Region….
- Select the 3D Growing Region… radio button (Figure 7).
- In the Algorithm drop-down menu, select Threshold (lower/upper bounds).
- Set the lower and upper thresholds to 0 and X% of the contralateral calf muscle signal, respectively (e.g., set the threshold to the value that will mask out the most speckle in the tumor ROI and will leave the most evaluable tumor T2(*)s).
- Set the ROI name as desired.
- Click on the image to place a seed for ROI growing.
- Click the Compute button.
- In the ROI menu, select Save All ROIs of this Series… (Figure 8).
NOTE: Now, the ROI defining the area to mask out of the parametric maps has been saved and can be applied to the parametric data. - Open the Parametric dataset in the 4D viewer.
- In the ROI menu, select Import ROI(s)….
NOTE: The mask ROI is now in the first parametric series. - Check that the ROIs are in the first 3D volume and not 4D.
- Apply mask to map the data. To do so, at the bottom of the ROI drop-down menu, select Set Pixel Values To. Then, select apply to: ROIs with same name… (Figure 9).
- Check the Propagate to 4D series box.
- Set pixels that are Inside ROIs.
- Set To this new value: as 0.
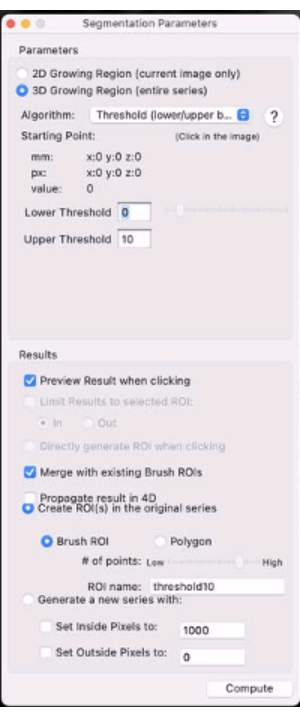
Figure 7: Screenshot showing the segmentation parameters. Please click here to view a larger version of this figure.
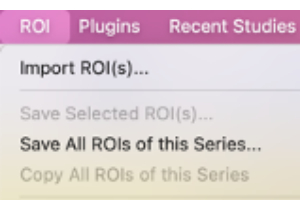
Figure 8: Screenshot showing how to select "Save All ROIs of this Series…". Please click here to view a larger version of this figure.
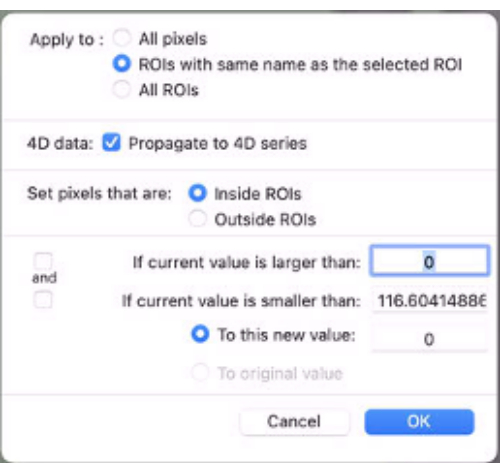
Figure 9: Screenshot showing the values to be inputted in "Set Pixel Values To". Please click here to view a larger version of this figure.
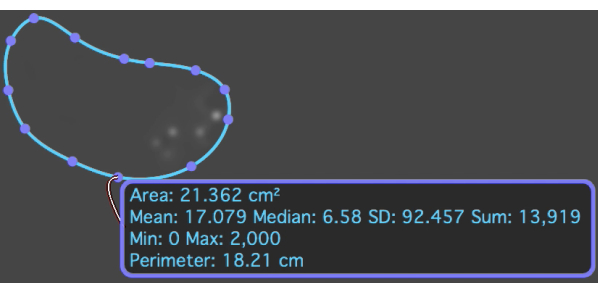
Figure 10: The T2* map with an ROI overlaid on the metastatic osteosarcoma lesion which shows the mean and standard deviation T2* value. Please click here to view a larger version of this figure.
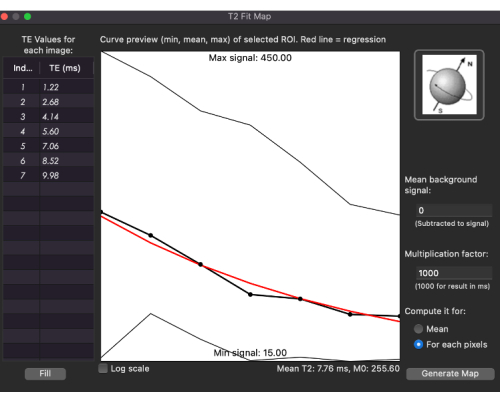
Figure 11: Fitting curve for T2* values for the T2* map in a patient with metastatic osteosarcoma. Please click here to view a larger version of this figure.
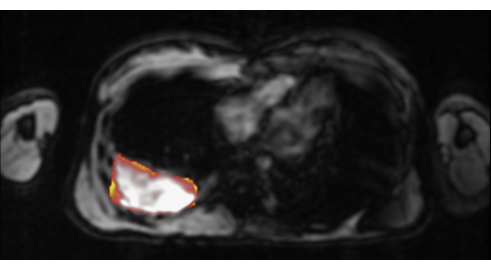
Figure 12: The T2* map overlaid on a T1-weighted image in this patient with metastatic osteosarcoma. Please click here to view a larger version of this figure.
The MRI scan was performed on a commercial scanner. An axial slice through the chest was imaged using a multi-echo single breath-hold gradient echo sequence with a range of TEs (1.22-9.98 ms). T2* was measured using this protocol from the ROI covering the whole tumor in all slices, avoiding the surrounding tissues. The T2* measurements were performed by two different observers. The mean of the measurements from all the slices were calculated for each observer. The tumor T2* relaxation rate was measured by placing an ROI to include the entire tumor tissue on a representative axial slice through the middle of the tumor tissue (Figure 10). Figure 11 shows a fitting curve generated with minimum, mean, and maximum T2* values for the selected ROIs with various TEs (ms) for this patient. The tumor T2* relaxation rate for our patient scan was 6.8 ms. For visual representation, the color-encoded T2* maps were merged with a contrast-enhanced T1-weighted gradient echo image for anatomical orientation (Figure 12). A positive result for this protocol will represent the T2* value in the specific tissue (Figure 10 and Figure 11).
