Representative results are shown in Table 1. The operation time was 112 min with a measured blood loss of 20 mL. The postoperative course was uncomplicated. The post-operative care was carried out in a regular hospital room. There was no need for an intensive care unit since there were no complications. A liquid diet was started after day one of the surgery – the patient did not report dysphagia. The patient was discharged in good condition on postoperative day 2, on a liquid diet. Soft food was gradually introduced, after day 5. The patient did not develop any complications during the follow-up. A barium esophagram was performed 30 days after surgery, (Figure 5). The exam showed an adequate emptying of the barium, with no contrast retention and a normal aspect of the fundoplication.
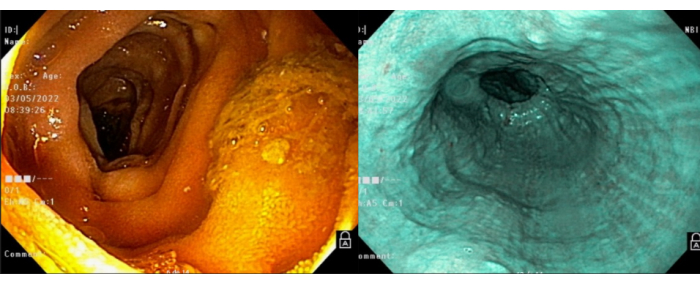
Figure 1: Endoscopy. The preoperative endoscopy showed no signs of malignancy or other diseases of the esophagus. Please click here to view a larger version of this figure.
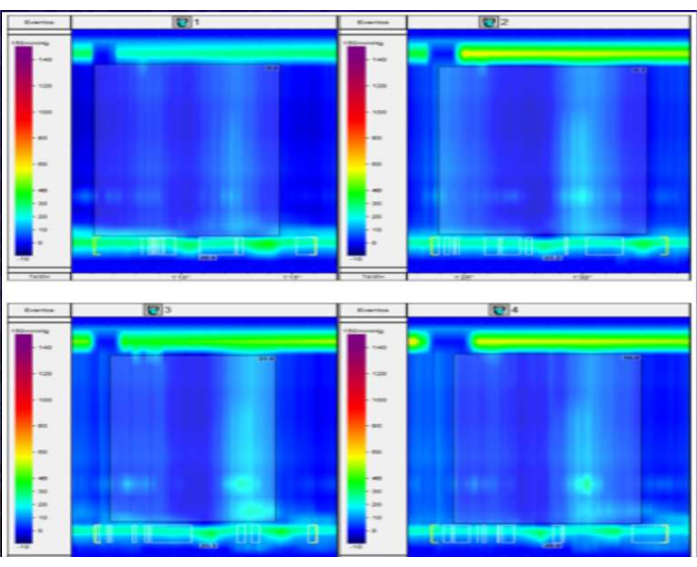
Figure 2: Manometry. This figure displays the results of a high-resolution esophageal manometry study in a patient with suspected esophageal motility disorder. The plot shows the pressure waves detected along the length of the esophagus during a series of swallows. In this case, there is a complete absence of peristaltic contractions and no detectable pressurization of the esophageal lumen. These findings are consistent with a diagnosis of achalasia type I. Please click here to view a larger version of this figure.
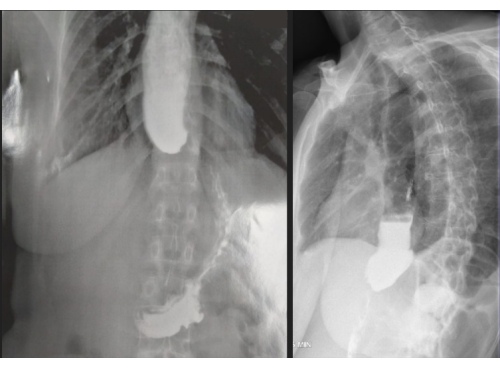
Figure 3: Barium esophagram. On the preoperative esophagogram, typical signs of achalasia were observed, including dilation of the distal esophagus, stasis of contrast material, and absence of air in the stomach. These findings are consistent with impaired esophageal emptying due to a failure of the lower esophageal sphincter to relax properly, which is characteristic of achalasia. The esophagus in this patient dilates up to 6 cm, indicating a grade III megaesophagus according to the Rezende-Mascarenhas classification. Please click here to view a larger version of this figure.
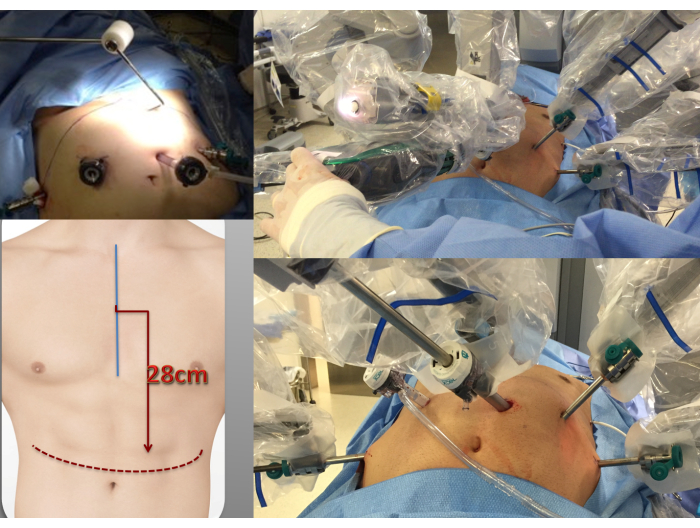
Figure 4: Trocar placement. The trocars are positioned in a linear arrangement directly above the umbilicus, with a distance of 28cm from the sternal angle. Please click here to view a larger version of this figure.
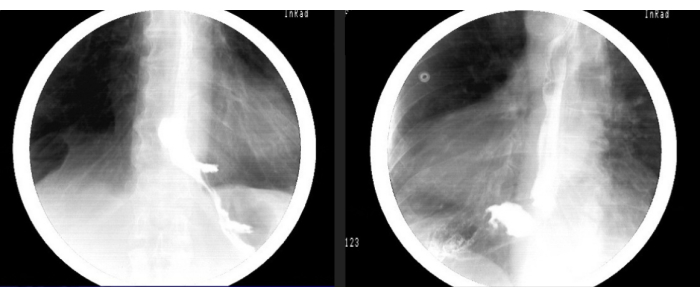
Figure 5: Postoperative barium esophagram. The postoperative esophagogram reveals improved contrast clearance from the esophagus to the stomach, along with a reduction in esophageal stasis. These findings suggest that the surgical intervention has been successful in improving esophageal motility and facilitating the emptying of ingested material into the stomach. Please click here to view a larger version of this figure.
| Operation time | 112 minutes |
| Blood loss | 20 ml |
| Hospital discharge | 2 days |
Table 1: Postoperative outcomes.
