A male patient aged 59 years old with symptoms including upper abdominal pain and jaundice was hospitalized in our department. He had no previous medical history and a relatively moderate normal body mass index (23.94 kg/m2). A contrast-enhanced CT scan was performed, and a tumor with a diameter of approximately 5.5 cm x 4.6 cm x 6.3 cm was found at the head and uncinate process of the pancreas (Figure 10). No evidence of distant metastasis was found, and percutaneous transhepatic cholangical drainage19 was performed before the operation. The total bilirubin declined from 201.4 µmol/mL to 36.0 µmol/mL.
Representative results are shown in Table 1. The operation lasted 314 min, and the total blood loss was 80 mL. The pancreatic fistula was not found, as the amylase level of the abdominal drainage fluid was normal throughout the postoperative period, and the drainage tubes were removed before postoperative day 8. No other significant morbidity occurred, and this patient was discharged on the 11th postoperative day. Histopathology confirmed a pancreatic intraductal papillary mucinous neoplasm with focal moderately differentiated invasive adenocarcinoma (Figure 11). The surgical margins were microscopically negative (R0), and none of the 18 lymph nodes were involved.
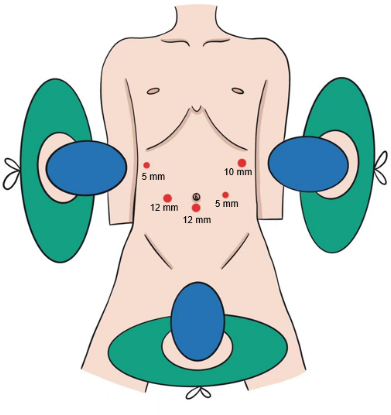
Figure 1: Distribution of the trocars. The five-port method was used. The patient was laid down in a supine position with his legs spread out. Please click here to view a larger version of this figure.
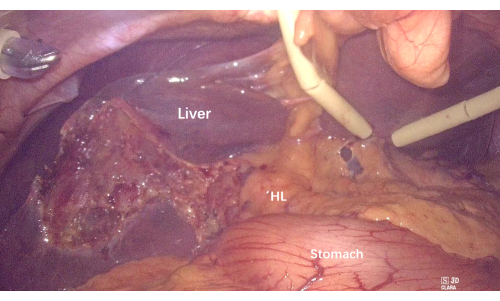
Figure 2: Removal of the gallbladder and suspending the liver to expose the hepatoduodenal ligament and hilum. Abbreviation: HL = hepatoduodenal ligament. Please click here to view a larger version of this figure.
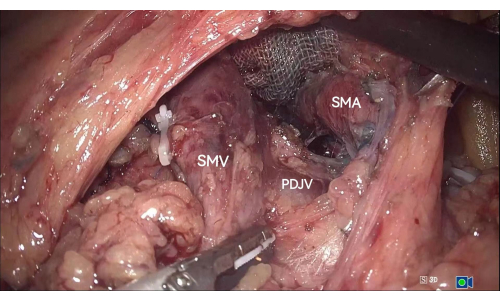
Figure 3: The PDJV between the SMV and the SMA is exposed in the inferior colonic region. Abbreviations: PDJV = proximal-dorsal jejunal vein; SMV = superior mesenteric vein; SMA = superior mesenteric artery. Please click here to view a larger version of this figure.
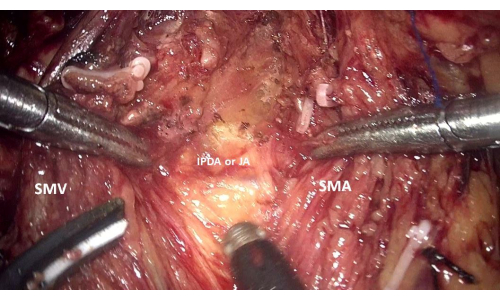
Figure 4: Exposure of the main branches of the IPDA and JA along the right side of the SMA through the median-anterior approach to the SMA. Abbreviations: IPDA = inferior pancreaticoduodenal artery; JA = jejunal artery; SMV = superior mesenteric vein; SMA = superior mesenteric artery. Please click here to view a larger version of this figure.
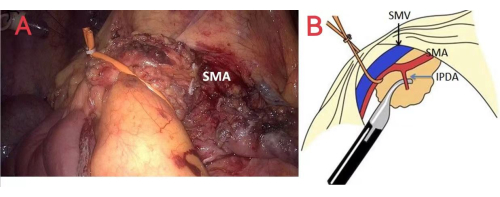
Figure 5: Method of hanging the SMA and SMV. (A) and (B) represent the method of hanging the SMA and SMV to establish a sufficient view of the left-posterior surface of the SMA. Abbreviations: IPDA = inferior pancreaticoduodenal artery; SMA = superior mesenteric artery; SMV = superior mesenteric vein. Please click here to view a larger version of this figure.
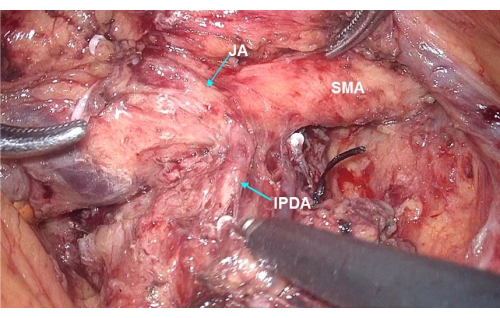
Figure 6: Dissection along the SMA circumferentially exposing the IPDA, which originates directly from the SMA. Abbreviations: IPDA = inferior pancreaticoduodenal artery; JA = jejunal artery; SMA = superior mesenteric artery. Please click here to view a larger version of this figure.
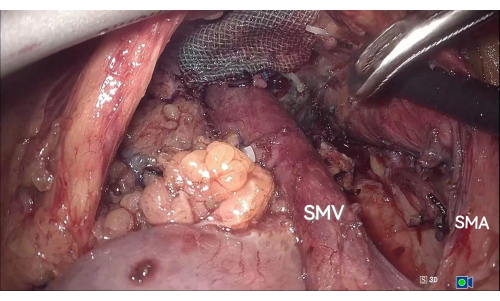
Figure 7: Separating the SMA and SMV from the uncinate process and mesopancreas. Using the median-anterior and left-posterior approaches to the SMA, the SMA and SMV are completely separated from the uncinate process and mesopancreas. Abbreviations: SMA = superior mesenteric artery; SMV = superior mesenteric vein. Please click here to view a larger version of this figure.
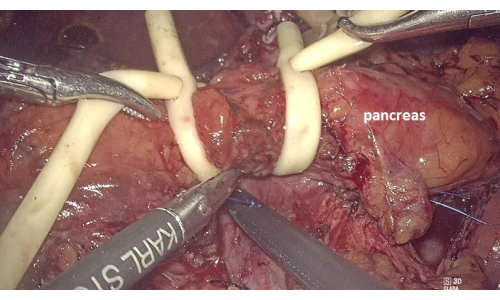
Figure 8: Placing two Fr14 catheters to block the pancreatic neck blood supply and reduce bleeding. Please click here to view a larger version of this figure.
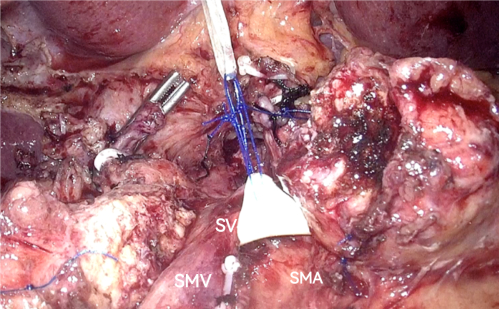
Figure 9: Suspending the SV to establish the exposure. Abbreviations: SV = splenic vein; SMA = superior mesenteric artery; SMV = superior mesenteric vein. Please click here to view a larger version of this figure.
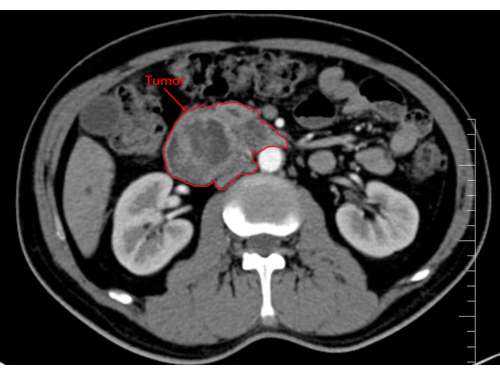
Figure 10: Image showing the tumor in the head and uncinate process of the pancreas. Please click here to view a larger version of this figure.
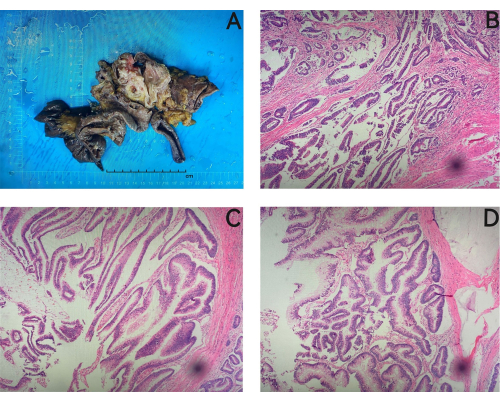
Figure 11: Histopathological study. Histopathology confirmed a pancreatic intraductal papillary mucinous neoplasm with focal moderately differentiated invasive adenocarcinoma. (A) Postoperative paraffin specimens in which the size of the stomach is 7 cm x 5 cm x 2.5 cm, the length of the small intestine is about 22 cm, the size of the pancreas is 6 cm x 4 cm x 3 cm, and there is a gray mass in the head of the pancreas, which is about 6 cm x 3 cm x 1.5 cm in size. (B) Atypical glands, suggesting a focally infiltrating adenocarcinoma. (C,D) An intraductal papillary mucinous tumor. Magnifications: B, 200x; C, 400x; D, 300x. Please click here to view a larger version of this figure.
| Variable | Outcome |
| Intraoperative | |
| operative time, min | 314 |
| Intraoperative blood loss, mL | 80 |
| Postoperative | |
| Postoperative pancreatic fistula | Not found |
| Drain removal, postoperative day | 8 |
| Postoperative hospital stay, days | 11 |
| Pathological diagnosis | Pancreatic intraductal papillary mucinous neoplasm with focal moderately differentiated invasive adenocarcinoma |
Table 1: Representative results of the surgery.
