Four sonographic windows are typically used to obtain the traditional FAST exam views19. The windows are subcostal 4-chamber (SC4C), right upper quadrant (RUQ), left upper quadrant (LUQ), and suprapubic/pelvic. Although the windows can be imaged in any order, the exam is typically performed in the following order: SC4C, RUQ, LUQ, and then suprapubic/pelvic1,19. This is because pericardial tamponade is usually more rapidly life-threatening than abdominal bleeding and because the RUQ view is the most sensitive site for the detection of fluid in the abdomen, regardless of the site of injury2. If the SC4C view is indeterminate for free pericardial fluid, the parasternal long-axis view can be added to the exam protocol, as explained below.
Subxiphoid (aka subcostal) 4-chamber (SC4C) and Parasternal Long-Axis (PLAX) views
The SC4C view is part of the imaging sequence for both the focused cardiac ultrasound and the FAST/e-FAST exams12,30. As part of the FAST/e-FAST exam, the main goal of the SC4C view is to screen for the presence of free pericardial fluid. When present, the fluid is typically present between the liver and the right ventricle, as shown in Figure 2B and Video 2. The presence of free pericardial fluid makes the SC4C FAST exam view "positive." In contrast, a "negative" SC4C FAST exam view is one that does not contain visible pericardial fluid, as shown in Figure 2A and Video 1.
Although traditionally, the SC4C view of the FAST exam has simply been scored either positive or negative for the presence of pericardial effusion1,31, some operators with advanced training in cardiac ultrasound may also be qualified to screen for specific signs of cardiac tamponade (e.g., right atrial collapse during ventricular systole, right ventricular collapse during ventricular diastole, etc.)27. But the minimum number of training studies required to accurately detect these specific signs of cardiac tamponade has yet to be defined32. And it is known that it typically takes a minimum of 30 cardiac ultrasound exams before a novice ultrasound user can even reliably detect the presence versus absence of pericardial effusion32. Given these issues, most FAST exam users should, at minimum, strongly consider cardiac tamponade when the following "sonographic Beck's triad" is present: (1) hypotension; (2) a moderate or larger pericardial effusion (> 1cm between the parietal and visceral pericardium); and (3) a fixed and dilated inferior vena cava (IVC)27,33. For details on image acquisition of the IVC, please see the relevant article by Hoffman et al.25.
Notably, at least two common conditions can be seen in the SC4C view that are easy to mistake for free peritoneal fluid: an epicardial fat pad and ascites. Classically, providers are taught that epicardial fat may be distinguished from pericardial fluid in the SC4C view as follows: (1) fat moves synchronously with the heart, whereas hemopericardium usually moves independently and (2) fat typically appears more "speckled" than does blood33 (Video 25). However, these criteria are highly subjective and thus prone to error, even by experienced providers34. Rather than relying on these subjective criteria, some authors have proposed adding the parasternal long-axis (PLAX) view to the FAST exam34, a step that we have found highly useful (Figure 3,4; Video 3,4). In the PLAX view, hemopericardium and epicardial fat pads are usually very easy to distinguish: epicardial fat lies anterior to the right ventricle, whereas hemopericardium typically settles in the most gravity-dependent portion of the view: between the descending thoracic aorta and the heart35 (Video 26).
In the SC4C view, ascites can also easily be misinterpreted as pericardial effusion. To differentiate the two conditions in the SC4C view, some sonographic clues can be helpful: pericardial fluid follows the contours of the heart, whereas ascites follows the contours of the liver and usually contains the undulating falciform ligament along the exact midline of the body36. However, these heuristics do not always provide a clear answer when evaluating the SC4C view alone. In these situations, peri-cardiac fluid that was visible in the SC4C view, fails to manifest in the PLAX view, and is likely peritoneal rather than pericardial.
For all of the above reasons, the PLAX view is a useful adjunct to the FAST exam, which typically only visualizes the heart in the subcostal window. Further, the PLAX view tends to be the easiest view for novice providers to obtain consistently37. In contrast, alternative cardiac views like the apical 4-chamber are consistently the hardest for ultrasound learners to obtain effectively37.
Right Upper Quadrant (RUQ) view
The RUQ view is considered "negative" when it reveals no free peritoneal fluid (Figure 6A; Video 5). In contrast, a "positive" RUQ exam is one that shows free fluid (Figure 6B; Video 7). Notably, in a supine patient, the most sensitive portion of this view and the entire FAST for fluid is around the caudal tip of the liver, so it is more important for providers to examine this location than the hepato-diaphragmatic interface29.
Left Upper Quadrant (LUQ) view
The LUQ view is considered "negative" when it reveals no free peritoneal fluid (Figure 8A; Video 10). In contrast, a "positive" LUQ exam is one that shows free fluid (Figure 8B; Video 12). Due to the presence of the spleno-colic ligament, free peritoneal fluid in the LUQ is more likely to be found in the spleno-diaphragmatic interface than in the spleno-renal interface2,29 (Video 12). So the search for fluid in the LUQ centers on visualization of the spleno-diaphragmatic interface. However, because some patients may have abnormal anatomy, it is reasonable to examine the spleno-renal interface, which sometimes requires a second LUQ view from one rib interspace caudal to the best spleno-diaphragmatic view.
In the LUQ, an important false positive for free peritoneal fluid is the presence of a full stomach (Video 28). If the stomach is distended with fluid or solids, it can be visualized inadvertently while insonating the LUQ window. This is more likely to happen if the ultrasound beam is angled too far anteriorly from the usual LUQ FAST exam angle. Anterior beam angulation creates two problems: (1) increases the chance of inadvertently visualizing the stomach and misinterpreting its contents as free peritoneal fluid, and (2) moves the beam away from the more gravity-dependent portions of the LUQ, where true peritoneal fluid is likely to be found. To decrease the chance of this anterior angulation, providers should aim the ultrasound beam posteriorly enough to be able to visualize the ipsilateral kidney.
Pelvic transverse and sagittal views
The female pelvic views are considered "negative" when they reveal no free peritoneal fluid (Figure 10A and Figure 13A; Video 15 and Video 20) and "positive" when they show free fluid (Figure 10B and Figure 13B; Video 18 and Video 21). Notably, in the female pelvis, free fluid is most likely to be found in the rectouterine space (pouch of Douglas) posterior to the uterus as well as the spaces lateral to the uterus. Free fluid is less likely to be found in the recto-vesical space because the peritoneal reflection between the bladder and uterus in women is shallow, whereas the peritoneal reflection posterior to the uterus tends to be deep enough to allow fluid to collect2.
Similarly, the male pelvic views are considered "negative" when they reveal no free peritoneal fluid (Figure 11A and Figure 14A; Video 16 and Video 22) and "positive" when they show free fluid (Figure 11B and Figure 14B; Video 19 and Video 23). In the male pelvis, free fluid is most likely to be found in the recto-vesical space posterior to the bladder. In this location, an important false positive for free fluid are the seminal vesicles, which are a normal finding38 (Video 16).

Figure 1: Probe positioning for obtaining the FAST exam version of the subxipoid (aka subcostal) 4-chamber view. Note that the probe indicator mark is pointing toward the patient's right side. Please click here to view a larger version of this figure.
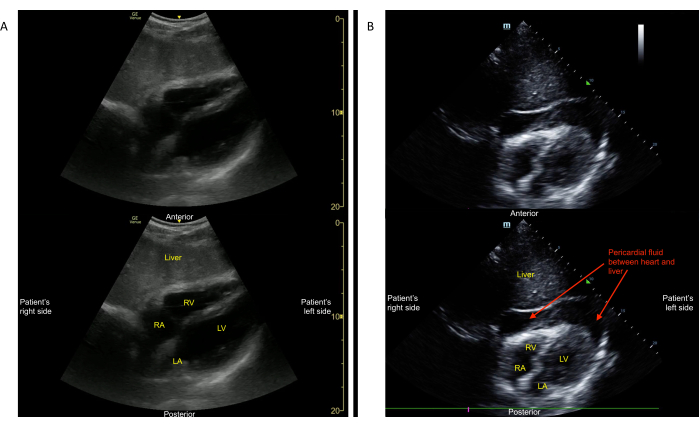
Figure 2: Subxiphoid (aka subcostal) 4-chamber view. (A) shows a grossly normal view. This view was obtained with a curvilinear probe in "abdominal" mode. The key structure that should be seen in the middle of this view is an image of the heart that includes the four cardiac chambers. In this example, there is no pericardial effusion seen around the heart (see Video 1). (B) shows the hemopericardium between the parietal and visceral pericardium. This view was obtained using a sector array probe (colloquially often referred to as a "phased-array" probe) and the view was obtained in "cardiac" mode, so the screen indicator is seen on screen right (see Video 2). Please click here to view a larger version of this figure.

Figure 3: Probe positioning for obtaining the FAST exam version of the parasternal long-axis view. Note that the probe indicator mark is pointing toward the patient's left hip. Please click here to view a larger version of this figure.
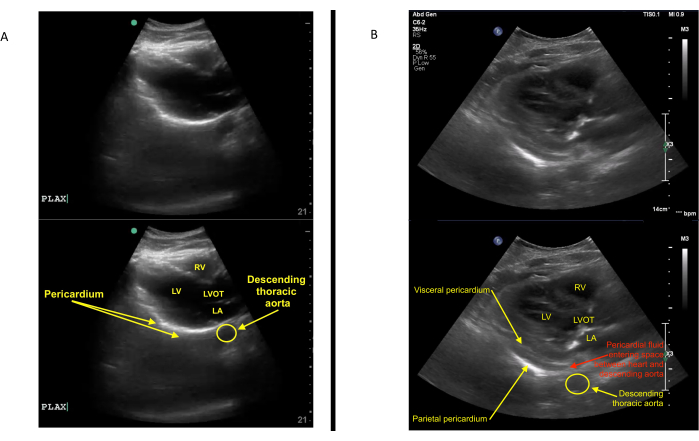
Figure 4: Parasternal long-axis view. (A) shows the grossly normal view. This view was obtained with a curvilinear probe in "abdominal" mode. The key structures that should be seen in this view are the following:descending thoracic aorta, left atrium (LA), left ventricle (LV), left ventricular outlow tract (LVOT), right ventricle (RV), and pericardium. There is no gross evidence of pericardial effusion between the pericardium and the descending thoracic aorta (see Video 3). (B) shows the fluid in the pericardial sac. The presence of the fluid between the heart and descending thoracic aorta identifies the fluid as in the pericardial rather than pleural space (see Video 4). Please click here to view a larger version of this figure.

Figure 5: Probe positioning for obtaining the FAST exam RUQ view. Note that the probe indicator mark is pointing cranially (i.e., toward the patient's head). Please click here to view a larger version of this figure.
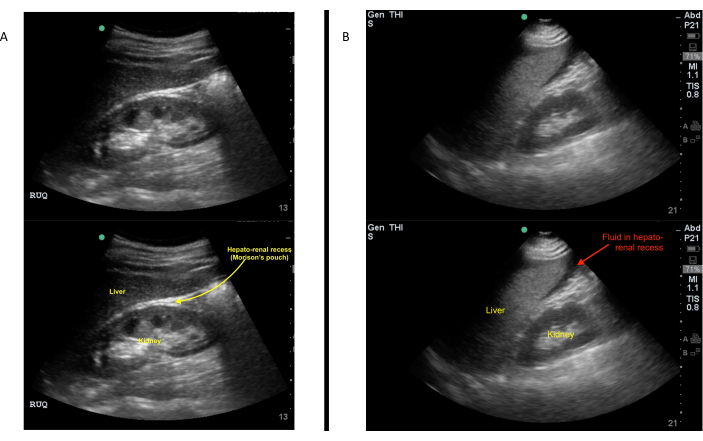
Figure 6: RUQ view. (A) shows the normal appearance of the RUQ view. This view includes the following three structures:(1) liver; (2) right kidney; (3) hepato-renal interface (a potential space also called Morison's pouch). (B) shows positive RUQ FAST exam highlighting free fluid between the liver and right kidney. Please click here to view a larger version of this figure.

Figure 7: Probe positioning for obtaining the FAST exam LUQ view. Note that the probe indicator mark is pointing cranially (i.e., toward the patient's head). Please click here to view a larger version of this figure.
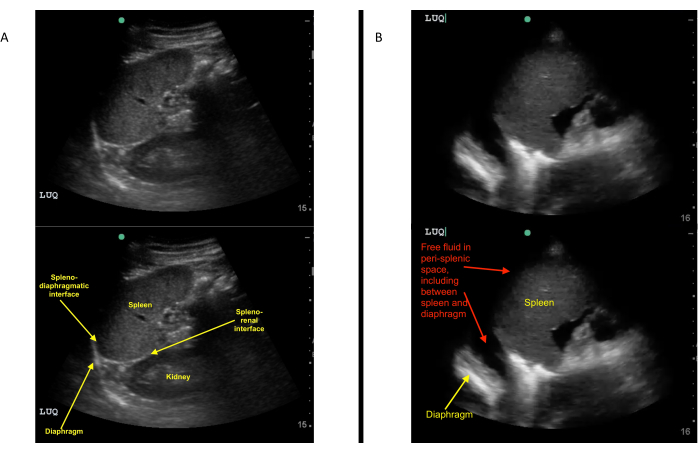
Figure 8: LUQ view. (A) shows the normal appearance of the LUQ view. This view includes the following three structures: (1) the spleen; (2) the diaphragm; and (3) the spleno-renal interface. (B) shows a positive LUQ FAST exam highlighting free peritoneal fluid between the spleen and diaphragm (see Video 12). Please click here to view a larger version of this figure.
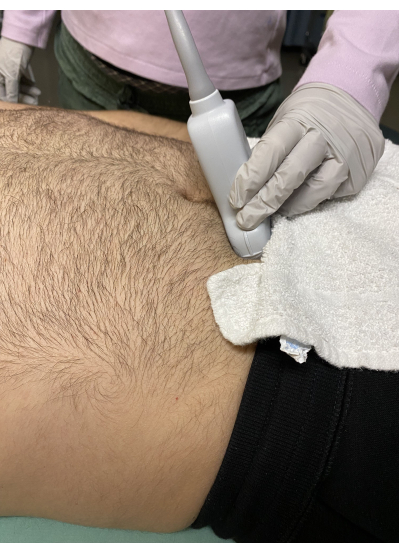
Figure 9: Probe positioning for obtaining the FAST exam suprapubic (aka pelvic) transverse view. Note that the probe indicator mark is pointing toward the patient's right side. Please click here to view a larger version of this figure.
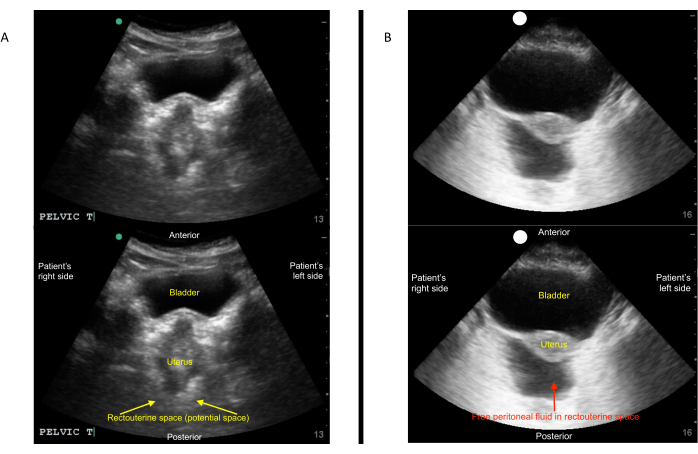
Figure 10: Pelvic transverse FAST exam view in a female. (A) shows normal appearance of the suprapubic (pelvic) transverse FAST exam view in a female. This view includes the following: (1) the bladder in its maximal dimension; (2) the uterus (if present); and (3) the space just posterior to the uterus (rectouterine pouch of Douglas). In women, the peritoneal reflection into the recto-vesical pouch is shallow. In contrast, the peritoneal reflection in the pouch of Douglas is relatively deep. Hence, the pouch of Douglas and the spaces lateral to the uterus are the most sensitive sites to screen for free peritoneal fluid in the female pelvis. (B) shows a positive pelvic transverse FAST exam view in a female showing free peritoneal fluid posterior to the uterus (pouch of Douglas). Please click here to view a larger version of this figure.
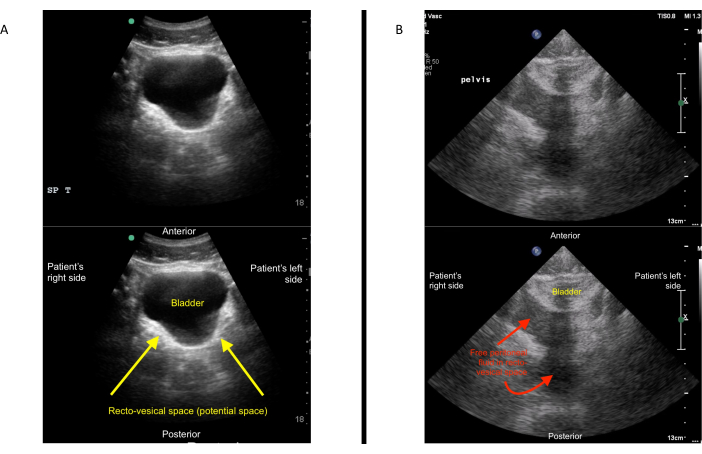
Figure 11: Pelvic transverse FAST exam view in a male. (A) shows normal appearance of the suprapubic (pelvic) transverse FAST exam view in a male. This view includes the following: (1) the bladder in its maximal dimension and (2) the space just posterior to the bladder (recto-vesical pouch). In men, the most sensitive site for detection of free peritoneal fluid is the recto-vesical space (i.e., the space just posterior to the urinary bladder). (B) shows a positive pelvic transverse FAST exam view in a male showing free peritoneal fluid posterior to the urinary bladder (recto-vesical space). Please click here to view a larger version of this figure.

Figure 12: Probe positioning for obtaining the FAST exam suprapubic (aka pelvic) sagittal view. Note that the probe indicator mark is pointing cranially (i.e., toward the patient's head). Please click here to view a larger version of this figure.
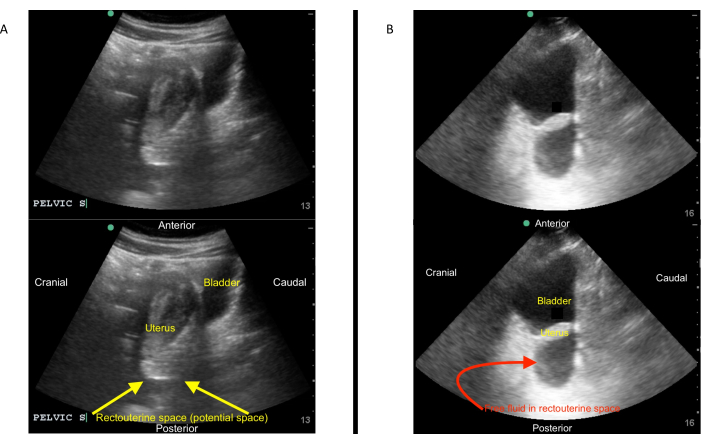
Figure 13: Sagittal FAST exam view in a female. (A) shows normal appearance of the suprapubic (pelvic) sagittal FAST exam view in a female. This view includes the following: (1) the bladder in its maximal dimension; (2) the uterus (if present); and (3) the space just posterior to the uterus (rectouterine pouch of Douglas). The sagittal pelvic view is an important feature of the exam because it is more sensitive to free fluid than the transverse pelvic view. (B) shows a positive pelvic sagittal FAST exam view in a female, highlighting free peritoneal fluid posterior to the uterus (pouch of Douglas). Please click here to view a larger version of this figure.
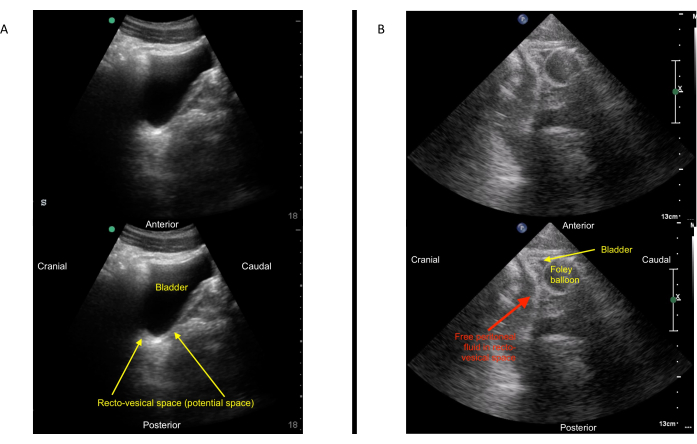
Figure 14: Sagittal FAST exam view in a male. (A) shows normal appearance of the suprapubic (pelvic) sagittal FAST exam view in a male. This view includes the following: (1) the bladder in its maximal dimension and (2) the space just posterior to the bladder (recto-vesical pouch). (B) shows a positive pelvic sagittal FAST exam view in a male highlighting free peritoneal fluid posterior to the urinary bladder (recto-vesical space). Please click here to view a larger version of this figure.
Video 1: Grossly normal subxiphoid (aka subcostal) 4-chamber view. This view was obtained with a curvilinear probe in "abdominal" mode. The key structure that is seen in the middle of this view is an image of the heart that includes the four cardiac chambers. In this example, there is no pericardial effusion seen around the heart. The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission. Please click here to download this Video.
Video 2: Subxiphoid (aka subcostal) 4-chamber view showing hemopericardium between the parietal and visceral pericardium. This view was obtained using a sector array probe (colloquially often referred to as a "phased-array" probe) and the view was obtained in "cardiac" mode, so the screen indicator is seen on screen right. The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission. Please click here to download this Video.
Video 3: Grossly normal parasternal long-axis view. This view was obtained with a curvilinear probe in "abdominal" mode. The key structures that are seen in this view are the following: descending thoracic aorta, left atrium (LA), left ventricle (LV), left ventricular outlow tract (LVOT), right ventricle (RV), and pericardium. No gross evidence of pericardial effusion between the pericardium and the descending thoracic aorta exists. The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission. Please click here to download this Video.
Video 4: Parasternal long-axis view showing fluid in the pericardial sac. The presence of the fluid between the heart and descending thoracic aorta identifies the fluid as pericardial rather than pleural. Left pleural fluid can also occasionally be seen in this view. To distinguish pericardial from pleural fluid in this view, it helps to assess the potential space between the descending thoracic aorta and the heart: pericardial fluid can enter into this space, whereas pleural fluid cannot. Please click here to download this Video.
Video 5: Normal appearance of the RUQ view. This view includes the following three structures: (1) liver; (2) right kidney; (3) hepato-renal interface (a potential space also called Morison's pouch). The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission. Please click here to download this Video.
Video 6: Demonstration of the operator fanning anteriorly to posteriorly and back in the RUQ view while centered on the hepato-renal interface. This fanning maneuver allows the operator to screen for fluid across a large three-dimensional interface between the liver and kidney, increasing the sensitivity of the exam for free peritoneal fluid. Please click here to download this Video.
Video 7: Positive RUQ FAST exam showing free fluid between the liver and right kidney. Please click here to download this Video.
Video 8: Cranial version of the RUQ FAST exam view. This view centers on the diaphragm and can be used to screen for fluid in the right pleural space as part of an e-FAST exam. Please click here to download this Video.
Video 9: Cranial version of the RUQ FAST exam view showing a large pleural effusion and lung consolidation cranial to the diaphragm. Please click here to download this Video.
Video 10: Normal appearance of the LUQ view. This view includes the following three structures: (1) the spleen; (2) the diaphragm; and (3) the spleno-renal interface.The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission. Please click here to download this Video.
Video 11: Demonstration of the operator fanning anteriorly to posteriorly and back in the LUQ view while centered on the spleno-diaphragmatic interface. This fanning maneuver allows the operator to screen for fluid across a large three-dimensional interface between the spleen and diaphragm, increasing the sensitivity of the exam for free peritoneal fluid. Please click here to download this Video.
Video 12: Positive LUQ FAST exam showing free peritoneal fluid between the spleen and diaphragm. Note the second clip in this video showing that, in the same patient, the spleno-renal interface appears to be devoid of fluid despite the copious fluid seen in the first clip between the spleen and diaphragm. Please click here to download this Video.
Video 13: The caudal version of the LUQ view centered on the spleno-renal interface. Please click here to download this Video.
Video 14: Cranial version of the LUQ FAST exam view. This view centers on the diaphragm and can be used to screen for fluid in the left pleural space as part of an e-FAST exam. Please click here to download this Video.
Video 15: Normal appearance of the suprapubic (pelvic) transverse FAST exam view in a female. This view includes the following: (1) the bladder in its maximal dimension; (2) the uterus (if present); and (3) the space just posterior to the uterus (rectouterine pouch of Douglas). In women, the peritoneal reflection into the recto-vesicle pouch is shallow. In contrast, the peritoneal reflection in the pouch of Douglas is relatively deep. Hence, the pouch of Douglas and the spaces lateral to the uterus are the most sensitive sites to screen for free peritoneal fluid in the female pelvis. The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission.Please click here to download this Video.
Video 16: Normal appearance of the suprapubic (pelvic) transverse FAST exam view in a male. This view includes the following: (1) the bladder in its maximal dimension and (2) the space just posterior to the bladder (recto-vesical pouch). In men, the most sensitive site for detection of free peritoneal fluid is the recto-vesicle space (i.e., the space just posterior to the urinary bladder)6. The schematic seen at the beginning and end of this clip was reprinted with author's (DC) permission. Please click here to download this Video.
Video 17: Demonstration of the operator fanning anteriorly to posteriorly and back in the male pelvic transverse view while centered on the bladder. This fanning maneuver allows the operator to screen for fluid across a large three-dimensional section of the recto-vesicle space, increasing the sensitivity of the exam for free peritoneal fluid. Please click here to download this Video.
Video 18: Positive pelvic transverse FAST exam view in a female showing free peritoneal fluid posterior to the uterus (rectouterine pouch of Douglas). Please click here to download this Video.
Video 19: Positive pelvic transverse FAST exam view in a male showing free peritoneal fluid posterior to the urinary bladder (recto-vesical space). Please click here to download this Video.
Video 20: Normal appearance of the suprapubic (pelvic) sagittal FAST exam view in a female. This view includes the following: (1) the bladder in its maximal dimension; (2) the uterus (if present); and (3) the space just posterior to the uterus (rectouterine pouch of Douglas). The sagittal pelvic view is an important feature of the exam because it is more sensitive to free fluid than the transverse pelvic view. Please click here to download this Video.
Video 21: Normal appearance of the suprapubic (pelvic) sagittal FAST exam view in a male. This view includes the following: (1) the bladder in its maximal dimension and (2) the space just posterior to the bladder (recto-vesical pouch). Please click here to download this Video.
Video 22: Demonstration of the operator fanning left to right and back in the male pelvic transverse view while centered on the bladder. This fanning maneuver allows the operator to screen for fluid across a large three-dimensional section of the recto-vesicle space, increasing the sensitivity of the exam for free peritoneal fluid. Please click here to download this Video.
Video 23: Positive pelvic sagittal FAST exam view in a female showing free peritoneal fluid posterior to the uterus (rectouterine pouch of Douglas). Please click here to download this Video.
Video 24: Positive pelvic sagittal FAST exam view in a male showing free peritoneal fluid posterior to the urinary bladder (recto-vesical space). Please click here to download this Video.
Video 25: Subcostal 4-chamber view showing a prominent epicardial fat pad. Please click here to download this Video.
Video 26: Parasternal long-axis views of the epicardial fat pad and hemopericardium. Please click here to download this Video.
Video 27: Subcostal 4-chamber view showing an example of ascites which could easily be mistaken for free peritoneal fluid. Please click here to download this Video.
Video 28: Left upper quadrant (LUQ) view showing a gastric body distended with fluid, a false positive finding when searching for free peritoneal fluid in the LUQ. Please click here to download this Video.
