The proposed method for LPS instillation in mice was verified by evaluating the expression of the inflammatory cytokine TNF-α and the lung dry-wet weight ratio 12 h after LPS instillation. There were four groups in the experiment: blank control (without any treatment), surgical intubation16, intranasal17,18, and noninvasive oropharyngeal intubation (n = 6). Compared with the blank control group, the serum TNF-α levels in the noninvasive oropharyngeal intubation group were significantly increased (Figure 8A). The lung dry-wet weight ratio was also increased (Figure 8B), reaching the same level as that in the surgical tracheal intubation group. The datasets were statistically analyzed with an unpaired ANOVA and post-hoc multiple-comparisons Tukey Kramer tests. All data are presented as mean ± SEM, and a level of p < 0.05 was considered statistically significant.
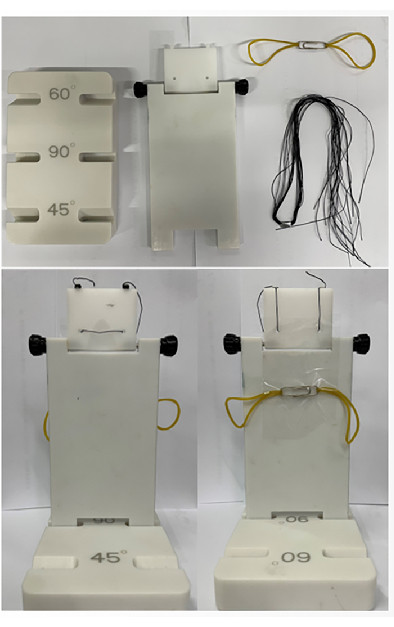
Figure 1: Intubation platform fittings and assembly. The platform consists of a base, a riser, a paper clip, two rubber bands, and some strings. Please click here to view a larger version of this figure.
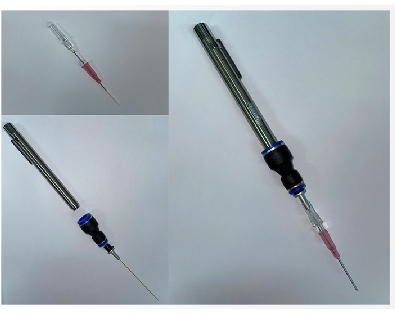
Figure 2: Intubation kit. This figure shows the intubation kit and its assembly. This includes a pen lamp, an optical fiber, and a cannula. Please click here to view a larger version of this figure.

Figure 3: Mouse fixation. Please click here to view a larger version of this figure.
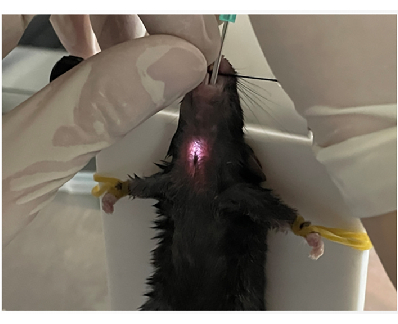
Figure 4: Locating the trachea. Please click here to view a larger version of this figure.
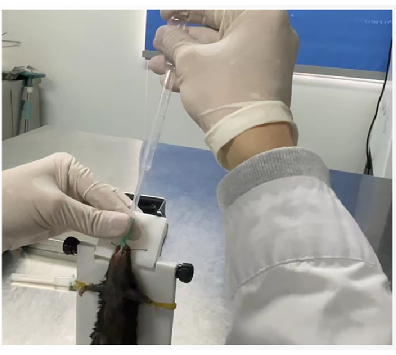
Figure 5: Pasteur pipette pump verification. Please click here to view a larger version of this figure.
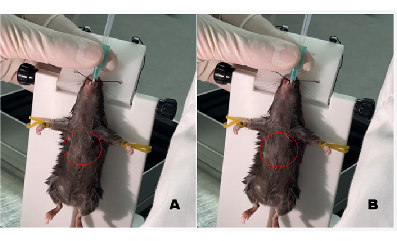
Figure 6: Before and after image of the chest showing successful intubation. (A) Chest before intubation. (B) Chest after intubation; the area showing the bulging of the chest is marked with a red circle. Please click here to view a larger version of this figure.
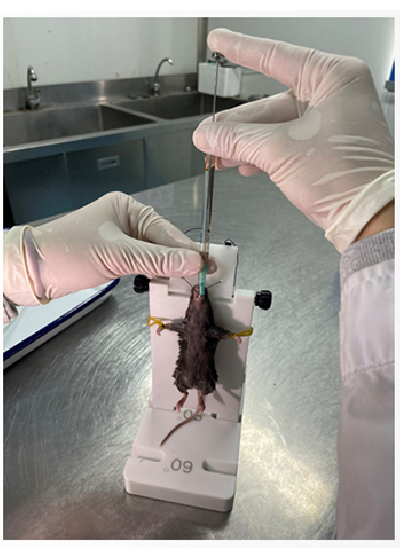
Figure 7: Flat head microsampler for delivering LPS. Please click here to view a larger version of this figure.
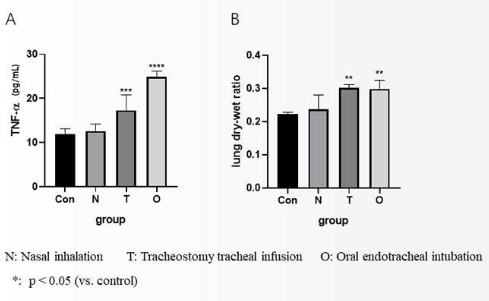
Figure 8: Assessment of the validity of the noninvasive LPS instillation. (A) Expression of TNF-α in the serum of C57BL/6 mice 12 h after an endotracheal injection of LPS. (B) Data analysis of the lung tissue dry-wet weight ratio. Please click here to view a larger version of this figure.
