The physical activity of rats was observed to evaluate the success or failure of the FS model. A previous study showed that cast immobilization significantly reduced the distance traveled and walking speed compared to normal rats17. Another research suggested that FS did not affect the distance traveled, and limping was the most common presenting symptom13. This study showed stiffness in the right shoulder joint, contraction of the right upper limb, muscular atrophy and limping in rats after modeling. These lesions in the MT and MO groups were resolved completely by 2 weeks of intervention. But there was no significant change in the M group.
The primary criterion for evaluating the effectiveness of Tuina in FS is the measurement of glenohumeral ROM18. We observed that the average values of glenohumeral ROM were 149.3° ± 5.9° in the C group, 111.1° ± 3.9° in the M group, 128.5° ± 2.8° in the MT group, and 119.56° ± 2.9° in the MO group. As depicted in Figure 7, the glenohumeral ROM of rats in the M group was significantly lower than that in the C group (P < 0.0001). Moreover, the ROM in the MT group and MO group was significantly higher than that in the M group (P < 0.05, P < 0.0001). However, the ROM in the MO group was significantly lower than that in the MT group (P < 0.0001). This finding suggests that Tuina can significantly improve shoulder joint function in FS rats.
Additionally, H&E staining and Masson staining can further demonstrate the effects of Tuina in preserving the structure and reducing fibrosis in capsule. To facilitate observation, the capsule of the glenohumeral joint was used for histological findings. The shoulder joint capsule comprises synovial and fibrous layers19. H&E staining revealed synoviocyte proliferation, flattened synovial folds, erythrocyte stasis, and vascular proliferation in the M group, which are typical features of FS (Figure 8A,B). These features diminished to some extent after Tuina and oral dexamethasone therapy (Figure 8C,D). Compared to the MT group, the MO group also showed much synovial cells. Masson staining showed the arrangement of fiber bundles in each group (yellow arrows). The capsule comprises a loose network of reticular fibers with fiber bundles arranged in a neat direction (Figure 8E). In the M group, the fiber bundles were arranged disorderly, indicating capsule fibrosis (Figure 8F). The capsules of rats in the MT group showed that the fiber bundles are neatly and clearly stratified but remain slightly disordered in the MO group (Figure 8G,H).

Figure 1: Protocol for establishing the FS model and Tuina intervention. The rats were on adaptive feeding for 7 days, FS model establishment for 21 days, and Tuina therapy was performed daily for 14 days. On day 36, all rats were sacrificed. Please click here to view a larger version of this figure.
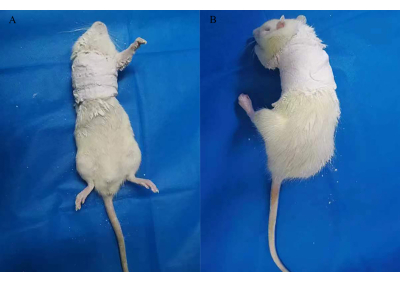
Figure 2: Cast immobilization for establishing a rat model of FS. Please click here to view a larger version of this figure.
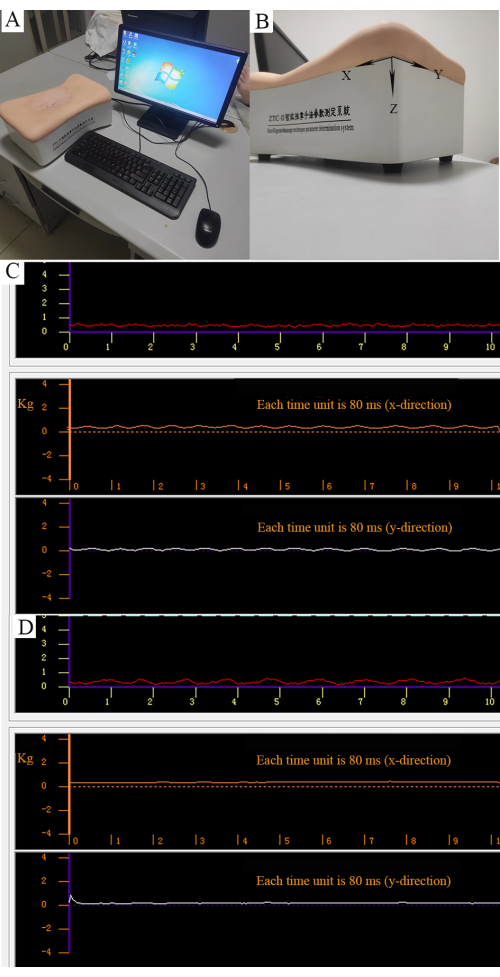
Figure 3: Quantitative control of manipulation. (A) Intelligent massage technique parameter determination system. (B) Three forces can be measured as parallel force along the X direction, longitudinal force along the Y direction, and vertical force along the Z direction. (C) Strength of the rotatory-kneading method. The red curve represents the stabilized vertical force (0.5 kg). The orange curve represents the regular parallel force. The white curve represents the regular longitudinal force. (D) The strength of the point-pressing method. The red curve represents the vertical force (0.5 kg). Orange and white curves represent nonparallel and longitudinal forces. Please click here to view a larger version of this figure.

Figure 4: Manipulation used in Tuina therapy. (A-C) Knead muscles of the right shoulders, forelimbs, and back. (D-G) Point-press LI15, SI11, HT01, and LI11. (H-K) Stretch the forelimb in adduction, abduction, anterior extension, and posterior extension positions. Please click here to view a larger version of this figure.
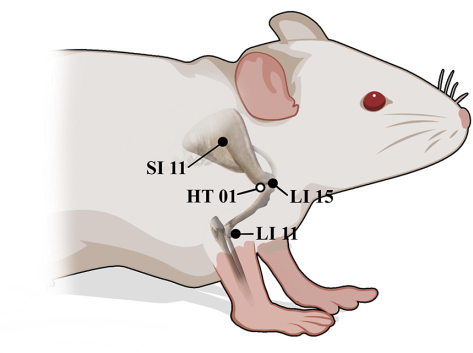
Figure 5: Anatomical positions of LI15, SI11, HT01, and LI11 in rats. ● Lateral surface, ○ Medial surface. Please click here to view a larger version of this figure.
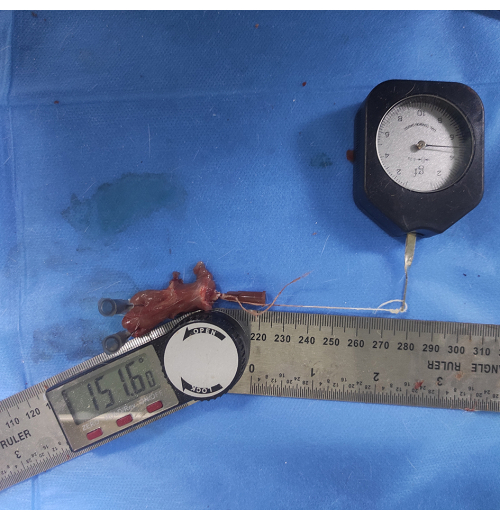
Figure 6: Measurement of glenohumeral ROM. A thin thread is attached to an injection needle inserted into the humeral shaft and pulled at the other end with a 5 g force to make it parallel to the humeral shaft. The angle between the lower edge of the scapula and the humeral shaft is measured as glenohumeral ROM. Please click here to view a larger version of this figure.
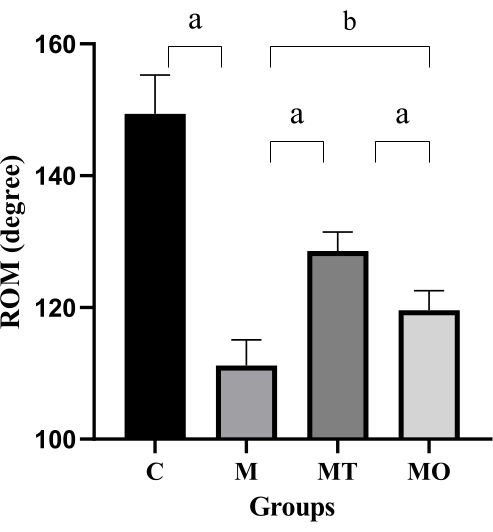
Figure 7: Glenohumeral ROM across three groups of rats. Values are means ± S.D., n = 5. Significant differences are indicated by one-way ANOVA (aP < 0.001 and bP < 0.0001). Please click here to view a larger version of this figure.
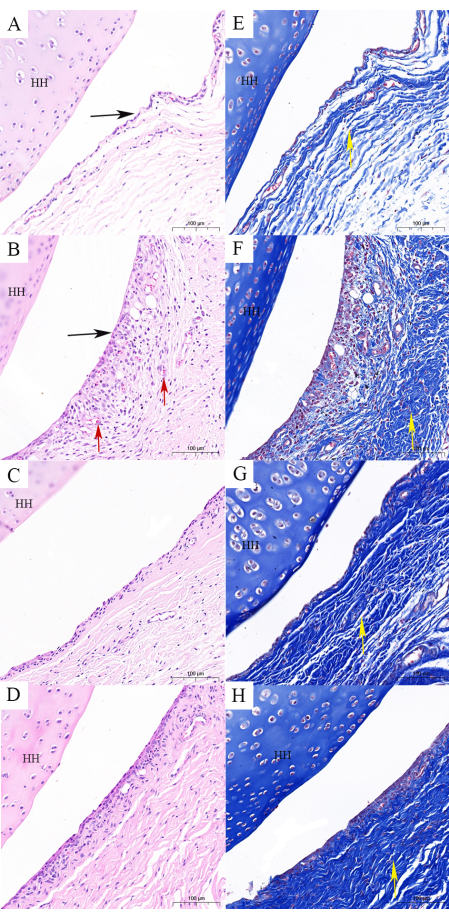
Figure 8: Histological findings of the shoulder capsule. (A,E) The control group contains a normal capsule structure (H&E and Masson staining). (B,F) The FS model group illustrates changes in the structure of the capsule as follows: flattened synovial folds, capsule fibrosis, and disturbed fiber bundles (H&E and Masson staining). (C,G). The FS model combined with Tuina group illustrates that the structure of the capsule is close to normal, and fibrosis is not obvious (H&E and Masson staining). (D,H) The FS model combined with oral dexamethasone shows that the structure of the capsule is close to normal, and fibrosis is obvious (H&E and Masson staining). Scale bar = 100 µm. HH: head of the humerus; black arrow: synovial folds; red arrow: erythrocyte stasis and vascular proliferation; yellow arrow: fiber bundles. Please click here to view a larger version of this figure.
| 4% paraformaldehyde | Solarbio | P1110 | |
| Embedding machine | Changzhou Paisijie Medical Equipment Co., Ltd | BM450A | |
| Ethylene Diamine Tetraacetic Acid (EDTA) | Solarbio | E1171 | |
| Hematoxylin eosin (HE) staining kit | Sparkjade | EE0012 | |
| Intelligent-massage technique parameter determination system | Shanghai Dukang Intrument Equipment Co. Ltd | ZTC- |
|
| Microtome | Leica | 531CM-Y43 | |
Modified Masson Trichrome Staining Solution |
Shanghai yuanye Bio-Technology Co., Ltd | R20381-8 | Bouin 50 mL; lapis lazuli blue dye 50 mL; Hematoxylin (Mayer) 50 mL; acidic ethanol differentiation solution 50 mL; ponceau magenta dye solution 50 mL; phosphomolybdic acid solution 50 mL; aniline blue staining solution 50 mL; weak acid 50 mL |
| Tribromoethanol | Macklin | T903147-5 |
