Multi-Tracer Studies of Brain Oxygen and Glucose Metabolism Using a Time-of-Flight Positron Emission Tomography – Computed Tomography Scanner
Summary
Quantitative measurements of oxygen and glucose metabolism by PET are established technologies, but details of practical protocols are sparsely described in the literature. This paper presents a practical protocol successfully implemented on a state-of-the-art positron emission tomography-computed tomography scanner.
Abstract
The authors have developed a paradigm using positron emission tomography (PET) with multiple radiopharmaceutical tracers that combines measurements of cerebral metabolic rate of glucose (CMRGlc), cerebral metabolic rate of oxygen (CMRO2), cerebral blood flow (CBF), and cerebral blood volume (CBV), culminating in estimates of brain aerobic glycolysis (AG). These in vivo estimates of oxidative and non-oxidative glucose metabolism are pertinent to the study of the human brain in health and disease. The latest positron emission tomography-computed tomography (PET-CT) scanners provide time-of-flight (TOF) imaging and critical improvements in spatial resolution and reduction of artifacts. This has led to significantly improved imaging with lower radiotracer doses.
Optimized methods for the latest PET-CT scanners involve administering a sequence of inhaled 15O-labeled carbon monoxide (CO) and oxygen (O2), intravenous 15O-labeled water (H2O), and 18F-deoxyglucose (FDG)-all within 2-h or 3-h scan sessions that yield high-resolution, quantitative measurements of CMRGlc, CMRO2, CBF, CBV, and AG. This methods paper describes practical aspects of scanning designed for quantifying brain metabolism with tracer kinetic models and arterial blood samples and provides examples of imaging measurements of human brain metabolism.
Introduction
The human brain is a heavy consumer of oxygen and glucose for metabolism. A proportion of glucose metabolism in the healthy human brain occurs outside of oxygen use, known as brain aerobic glycolysis (AG), the purposes of which are under intense investigation1,2,3,4,5. Prior studies in animal models and humans report an association between AG and development and aging, synaptic and neurite development, memory, amyloid deposition in Alzheimer's disease, and white matter function and disease1,6,7,8,9,10,11,12,13. Thus, there is ongoing interest in studying AG and other aspects of brain metabolism to better understand the human brain as it ages and incurs injury and disease.
At present, methods for evaluating human brain AG in vivo require PET imaging with multiple oxygen and glucose radiotracers to measure each of cerebral metabolic rate of glucose (CMRGlc)14, cerebral metabolic rate of oxygen (CMRO2)15, cerebral blood flow (CBF)16, and cerebral blood volume (CBV)17. Beyond imaging, quantitatively measuring brain metabolism with PET requires other complexities, including evaluating the arterial input function, typically via invasive arterial cannulation and sampling; ensuring that participants precisely follow instructions for radiotracer inhalation while restricting head motion; handling of radiotracers with very short half-lives (2 min) safely and effectively; managing large datasets; and performing advanced analytical methods to calculate metabolic parameters accurately. Also notable are the limitations of using [18F]FDG for the estimation of CMRGlc5,14.
This protocol addresses practical matters most relevant for the successful measurements of quantitative brain metabolism in our experience. This protocol includes a description of essential procedures and cautionary notes for avoiding common errors. It defers careful discussion of more general principles of metabolism, neuroscience, imaging, tracer kinetics, and methods of inference from radiotracer PET imaging. The intended audience includes novices to metabolic measurements using PET, as well as more experienced PET researchers and clinicians interested in employing 15O radiotracers. This protocol assumes familiarity with human imaging studies, invasive medical procedures, radiotracers, and quantitative methods of inference. Numerous, excellent references exist on brain PET imaging in general18, and for 15O-oxygen PET more specifically19. For [18F]FDG, as well as other practical matters of performing PET, Turku PET Centre provides valuable reference materials as well as links to the extensive primary research literature20.
The protocol sections commence with relevant considerations with regard to participant selection that are essential for compliance and successful scanning. Next, the protocol outlines aspects pertaining to supportive scanning with MRI for neuroanatomy. Next, the protocol describes clinical laboratory orders that include measures important for the quantification of oxygen and glucose metabolism. Next, the protocol lists matters involving the cyclotron and delivery of radiopharmaceuticals. Descriptions merely take the perspective of investigators working at the point of care in the imaging facility, omitting considerations required of cyclotron facilities and staff. Next, the protocol details the preparing and managing of arterial lines. Establishing and maintaining arterial lines require meeting compliance criteria specific to institutions, and the protocol outlines successful workflows. Next, the protocol provides the essential operational procedures for scanning with PET, including details of participant positioning, CT for attenuation correction, administration of radiopharmaceuticals, and performing arterial measurements. Venous sampling discusses potential alternatives to arterial sampling in measurements of CMRGlc with [18F]FDG. A section on PET image reconstruction and data storage details software parameters and practical matters of information technology. The section on discharge and participant follow-up notes essential communications for participant safety. Important calibration activities are also discussed. Many suitable analysis methods and kinetic models are well described in published scientific reports and their numerous antecedents; thus, this protocol largely directs the reader to references of published approaches. Representative results illustrate the successful implementation of protocols. The discussion section elaborates advantageous aspects and limitations of the protocol, its potential in human neuroscience, and matters pertaining to safety.
Protocol
NOTE: The Institutional Review Board and Radioactive Drug Research Committee of Washington University School of Medicine approved all studies based on the protocol described below. All human participants provided informed written consent prior to participating in research studies based on the protocol below. See the Table of Materials for details related to all equipment, materials, and reagents used in this protocol.
1. Participant Selection
- Inclusion criteria
- Include only adult participants. Ensure participants can follow study procedures, including instructions for the inhalation of radiopharmaceutical gases, and are able to provide informed consent or assent with appropriate surrogate consent. Ensure participants can undergo imaging in the supine position for up to 2-3 h with breaks, and continuously for 60 min without breaks.
- Exclusion criteria
- Exclude participants who have contraindications to radioactive drug research, such as pregnancy at the time of PET. Exclude participants with contraindications to MRI, since MRI is required for anatomic image registration, spatial normalization, and partial volume correction.
- Exclude participants with any contraindication to radial artery cannulation when radial artery cannulation is to be performed. Exclude participants with significant anemia or who have recently donated blood products, since invasive arterial sampling results in a total blood volume loss that can exceed 100 mL.
- Exclude participants with significant pulmonary diseases as their capacity to successfully inhale and exchange labeled [15O]O2 and [15O]CO in the lungs may be impaired. Exclude individuals with ongoing medical illnesses beyond those of interest, which are expected to significantly alter cerebral metabolism and blood flow.
NOTE: This is dependent on the specific aims and targets of a particular project, for example, if the project is focused on healthy aging, large strokes or sickle cell anemia may be among the exclusion criteria. - Exclude participants who cannot achieve a blood glucose level below 165 mg/dL prior to the administration of [18F]FDG.
2. MRI for neuroanatomy
- Schedule MRI in advance of PET scanning. Ensure an MRI protocol for a 3T scanner that includes a magnetization prepared rapid gradient echo (MPRAGE) pulse sequence with isotropic 0.8-1.0 mm resolution and, ideally, prospective methods for motion correction21.
NOTE: Prospective motion correction provides additional optimization of T1w anatomy for use in fusion with PET imaging, but the omission of prospective motion correction is unlikely to be highly consequential for current PET imaging in participants who are adherent to avoiding head movement. High-quality T1w anatomy is significant for partial volume correction of PET22,23. - Acquire neuroanatomical MRI for regional parcellations and segmentations, atlas registrations, and partial volume corrections. Verify successful neuroanatomical MRI before scheduling and subjecting a participant to invasive arterial lines and radiopharmaceuticals.
3. Laboratory orders
- Order arterial blood gases, hemoglobin, hematocrit, and plasma glucose from clinically certified laboratories. Order quantitative oxyhemoglobin, carboxyhemoglobin, and methemoglobin for smokers and those with medical conditions associated with altered hemoglobins.
- Measure pulse oximetry using validated devices, such as those designed for critical medical care.
4. Delivery of radiopharmaceuticals
NOTE: Measuring brain oxygen metabolism and AG with PET requires a cyclotron facility capable of producing and delivering 15O radiopharmaceuticals, which have 122 s half-lives. Transport of radiopharmaceuticals between the cyclotron facility and PET scanner must be sufficiently and reliably rapid to provide adequate dosing at the time of radiotracer administration.
- Ensure that all radioactivity dose calibrators have power and allow time for sufficient instrument warm-up (typically, at least 60 min).
- For gaseous radiopharmaceuticals, position a shielded gas canister and its incorporated pico-ammeter dose calibrator near the PET gantry of the PET scanner. Ensure secure attachments of sterilized expandable bellows, particulate filter, large-diameter plastic polymer tubing, clamp, and disposable mouthpiece. See Figure 1.
- Complete quality assurance procedures for nylon gas lines, 1/8 inch inner diameter, under exhaust, from the cyclotron for delivery of [15O]CO and [15O]O2. Complete quality assurance of purified hydrogen sources and processing units for generating radiopharmaceutical [15O]H2O as a derivative of [15O]O2, for subsequent injection. See Figure 1.
5. Arterial lines
- Placement and management
- Cannulate the radial artery by consultation with a physician with specialty training for routine placement of arterial lines, for example, interventional radiology, anesthesiology, or critical care medicine.
- Make available an ultrasound device with a probe appropriate for imaging the radial artery.
- Supply the interventional physician with their preferred consumables for arterial line placement, most commonly, a kit with a guidewire that implements the Seldinger technique.
- Make every effort to insert the angiocatheter in the participant's non-dominant hand.
- Evaluate and manage the participant throughout radial artery cannulation using the services of an experienced nurse or equivalent healthcare professional.
- Ensure collateral arterial circulation of the hand by ultrasound.
- Prepare and manage the sterile field during arterial cannulation.
- Assist the interventional physician with sterile cannulation procedures.
- Prime rigid pressure lines and supply normal saline pressurized to 300 mm Hg.
- Perform continuous arterial line management during the 2-3 h protocol, including routine monitoring of arterial pressure waveforms and manipulation of arterial line circuits. For continuous arterial sampling, switch in-line stopcocks from supplying back pressure for the radial artery to extraction of arterial blood by peristaltic pumping to flushing and maintaining radial artery access. When priming line segments that never flow into the radial artery, flush with heparinized solutions (up to 10 U/mL) to help maintain patency.
NOTE: Minimize using heparin when possible for maintaining the radial artery catheter given the uncertain evidence of its efficacy and to avoid the risk of provoking heparin-induced thrombocytopenia. - Use a moldable, yet rigid, arm board to help secure the radial artery catheter and lines. Ensure that repeated manipulations of stopcocks do not disturb the radial artery catheter.
- Confirm normal arterial pressure waveforms prior to each radiotracer administration to ensure patency of the radial artery catheter.
- Cannulate the radial artery by consultation with a physician with specialty training for routine placement of arterial lines, for example, interventional radiology, anesthesiology, or critical care medicine.
- Gamma detectors for arterial samples
NOTE: Use a gamma detection probe device and peristaltic pump for arterial input function measurement. Although hand-drawn samples are feasible for [18F]FDG and other longer half-life radiotracers, employing a sequence of four rapid 15O scans is greatly facilitated by automated sampling using a peristaltic pump and a gamma detector sufficiently compact to place alongside the participant's hand.- Position arterial-line assemblies as close as feasible to the radial artery catheter to make measurements with minimal dispersion and delay at the gamma detection probe. Ensure that the path from the cannulation site through line assemblies to the gamma detection probe is consistent with calibration data available for the line assembly.
- Supply continuous power through an uninterruptible power supply to ensure the stability of photomultipliers for coincidence gamma detectors. For coincidence detection, use 100 ns timing windows and ensure that the nominal detection sensitivity is at least 2.4 cps kBq-1 mL-1 with <1% linearity through 10 kcps.
NOTE: Liquid-filled waveguides for coincidence detection are fragile, requiring care when handling and transporting from storage areas to the PET suite.
6. Scanning
- Minimize head movements
- Prior to scanning, educate the participant on the importance of avoiding head movements during scanning.
- Study participant positioning
- Ensure that PET-CT hardware and software configurations permit scanning with head-first or feet-first positioning of the study participant. Whenever possible, prefer feet-first positioning for PET, such that the participant's extremities and torso lie beyond the PET gantry, the participant's head remains centered within the PET gantry, and the CT gantry remains unoccupied (Figure 1).
- Guide and position the participant to lie on the lowered gantry table in accordance with all pre-existing protocols for human PET-CT scanning, such as ensuring recent urinary voiding, wearing appropriate garments, and removing eyeglasses, jewelry, or hair ornaments incompatible with the scanner.
- Ensure the integrity of all arterial and venous lines as the gantry table moves into the scanner bore. Ensure continuous connection of arterial lines with pressurized saline sources. Ensure disconnection of peristaltic pumps, gamma detection probes, and any other devices that cannot pass through the scanner bore and reconnection subsequently.
- Ensure the comfort of the participant, especially adequate cushions for positioning of head, neck, spine, hips, and leg flexion. Ensure comfortable head positioning upon freely positioning foam headrests, and then secure the participant's forehead to the gantry table with elastic, self-adhesive, self-removable wrapping as a reminder to the participant to avoid head motion. Ensure sufficient blankets for thermal comfort. Confirm the participant's understanding of the necessity of avoiding head movement throughout CT and PET scanning.
NOTE: The headrests and elastic wrapping substantially limit head motion even in cognitively impaired participants. - Ensure that the gantry table passes through the scanner bore until the participant's extremities and torso lie beyond the CT gantry and the participant's head is centered in the CT gantry. Align the participant's canthomeatal line with vertical laser markers upon entry into the CT gantry, then angle the chin slightly inferiorly. Perform CT as described below. Confirm on CT that this positioning captures the entire cerebrum and cerebellum within the PET field-of-view.
- Ensure that the gantry table continues through the scanner bore until the participant's head is centered in the PET gantry. Ensure adequate access to arterial and venous lines as well as adequate wrist extension to accommodate the radial artery cannulation. Ensure that ceiling exhaust vents can effectively remove inadvertently exhaled radiotracer gases near the edge of the PET gantry. Perform CT and PET as described below in steps 6.3-6.5.
- Routinely monitor the participant during PET, assessing the participant's comfort with minimal verbal communication during scanning.
NOTE: Feet-first positioning facilitates the administration of radiotracer gases with improved communications and improved manipulations of inhalation tubing. However, for most gantry tables, feet-first positioning may be incompatible with using thermoplastic head-retention masks. Feet-first positioning may also be incompatible with devices that shield the head from emissions originating from the body inferior to the head. Such shields can otherwise reduce randoms originating from the body.
- CT for attenuation correction
- Obtain a low radiation-dose head CT appropriate for attenuation correction. If the participant requires a break during scanning and leaves the scanner, repeat the CT scan prior to resuming the PET session to allow for console-based reconstruction of subsequent PET imaging. Useful CT parameters include tube current 75 mA, rotation time 0.5 s, spiral pitch 1.5, and tube voltage 120 kVp, with vendor-recommended convolution kernels and reconstruction to 512 x 512 x 88 matrix, 0.98 x 0.98 x 3.00 mm3 resolution.
- Administration of gaseous radiopharmaceuticals
- Instruct participants on the procedure of inhalation prior to the first gas administration, with emphasis on inhaling and exhaling through the tube and not breathing through their nose.
- Prepare the shielded gas-storage container equipped with a pico-ammeter dose calibrator. Within the gas container, connect expandable bellows to the rigid narrow-diameter nylon line from the cyclotron as well as to a semi-rigid large-diameter plastic polymer tube that is kept clamped except during administration. Place a virus-capturing particulate filter in line with the large-diameter tube according to infection control requirements formulated for the Covid-19 pandemic. Attach a disposable plastic mouthpiece to the end of the tubing.
- Request that the cyclotron facility deliver gaseous radiopharmaceuticals to the gas container.
- Prepare to administer all gaseous radiopharmaceuticals as boluses. The procedure for inhalation is identical in all cases.
- Monitor the activity of each gas delivered to the expandable bellows to peak activity, and then wait for the activity to fall below the maximum dose allowed by the Radioactive Drug Research Committee (55 mCi). Monitor activities using pico-ammeter dose calibrators. Initiate scanner acquisition of emissions.
- Commence scanning immediately prior to the start of inhalation to ensure the acquisition of the start of the time activity curve. Obtain 6-7 min of emissions with 3 s frames x 23, 5 s frames x 6, 10 s frames x 20, and then 30 s frames for the remainder of the scan.
- Instruct the participant to exhale fully and lower the participant's mask.
- Place the mouthpiece in the participant's mouth. Ask the participant to form a tight seal around the mouthpiece with their lips and then inhale as much as possible. Ask the participant to hold their breath for a few seconds to facilitate their lungs absorbing the gaseous radiopharmaceutical.
- Ask the participant to exhale again through the tube, blowing residual gaseous radiopharmaceutical back into the bellows. Re-clamp the tube and retrieve it from the participant.
- Monitor the gas activity in the bellows from the start of inhalation to the end of exhalation. Calculate the total administered dose by the difference in activities. Aim for the total administered dose to exceed 20 mCi.
- Administer one dose of [15O]CO. Monitor arterial measurements for nominal time activity curves. If arterial measurements are technically insufficient, administer a replacement dose of [15O]CO. Allow intravascular [15O]CO to attain steady state, requiring approximately 1-2 min17.
- Administer two sequential doses of [15O]O2. Monitor arterial measurements for nominal time activity curves.
NOTE: This procedure is robust even with mildly cognitively impaired participants. However, participants incapable of performing this procedure, due to severe cognitive impairment or facial weakness, are excluded to minimize the risk of inadequate radiotracer administration and leakage of gas into the ambient air during exhalation. For continuous administration and use of masks for scavenging gaseous radiotracers, consult alternative methods reported and referenced by Iguchi et al.24 Repetition of dosing [15O]O2 in duplicate is recommended because of the lower signal-to-noise ratios (unfavorable noise equivalent counts) typically obtained with [15O]O2.
- Administration of injected radiopharmaceuticals
- Request that the cyclotron facility deliver intravenous radiopharmaceuticals to the scanner bay.
- Prepare to administer all intravenous radiopharmaceuticals as boluses. The procedure for intravenous injection is similar for all cases.
- Monitor the dose in a well-counter dosimeter until it falls below the maximum allowable (25 mCi for [15O]H2O and 6 mCi for [18F]FDG).
- Commence scanning immediately prior to intravenous injection to ensure the acquisition of the start of the time activity curve. For [15O]H2O, obtain 6-7 min of emissions with 3 s frames x 23, 5 s frames x 6, 10 s frames x 20, and then 30 s frames for the remainder of the scan. For [18F]FDG, obtain 60 min of emissions with 3 s frames x 23, 5 s frames x 24, 20 s frames x 9, 60 s frames x 13, 300 s frames x 7, and a 351 s frame x 1.
- Promptly inject the intravenous dose. Measure the residual radioactivity in the syringe to calculate the administered dose by differences. Ensure that the total administered dose is not below the minimum dose allowed (15 mCi for [15O]H2O and 4 mCi for [18F]FDG).
- Monitor arterial measurements for nominal time activity curves. For [15O]H2O, if arterial measurements are technically insufficient, administer a replacement dose.
NOTE: Administration of [15O]H2O is in some respects simpler than the administration of gases as the former can be injected intravenously. However, due to the short half-life of [15O]H2O, this still requires careful orchestration, depending on the PET scanner location and where [15O]H2O is produced and obtained.
7. Arterial measurements
- After positioning the study participant in the scanner, prepare all devices needed for arterial measurements of radiopharmaceutical activities.
- Ensure the integrity of connections between the radial artery angiocathether, rigid pressure lines, stopcocks, pressurized bag for supply of normal saline, extension catheter sets for gamma detectors, and extension catheter sets for peristaltic pumps. Ensure correct priming so that no air bubbles can be introduced into the radial artery and that no air bubbles will interfere with peristaltic pumping for extracting arterial blood.
- For the gamma detector, use microbore catheter extension sets with no more than 48 cm length and no more than 0.6 mL priming volume.
- For the peristaltic pump, set the maximum allowable occlusion pressure limit.
- If the peristaltic pump is an infusion pump operating with reversed flow directions, select the minimum flow rate to keep vessel open (KVO).
- Ensure the integrity of connections between the radial artery angiocathether, rigid pressure lines, stopcocks, pressurized bag for supply of normal saline, extension catheter sets for gamma detectors, and extension catheter sets for peristaltic pumps. Ensure correct priming so that no air bubbles can be introduced into the radial artery and that no air bubbles will interfere with peristaltic pumping for extracting arterial blood.
- Immediately prior to administering radiopharmaceuticals, close the stopcock to the pressure bag and pressure monitor, and operate the pump at 300 mL/h. Confirm the extraction of blood from the radial artery and its passage through extension catheter sets for gamma detectors and extension catheter sets for the pump. Confirm continuous measurements of radiopharmaceutical activity in the gamma detectors throughout the bolus passage of radiopharmaceuticals through the arterial circulation25.
- Verify simultaneous acquisition of time activity curves from the PET scanner.
- Continue pumping at 300 mL/h and verify measurements of radiopharmaceutical activity in the gamma detectors for at least 300 s after inhalation of [15O]CO, 120 s after inhalation of [15O]O2, 120 s after injection of [15O]H2O, and 300 s after injection of [18F]FDG.
- For [18F]FDG, continue pumping blood at reduced pump rates no lower than 20 mL/h until the end of PET scanning.
- After each arterial measurement, reconfigure the arterial lines to flush the radial artery catheter; then, flush the line circuit that supplies the gamma detectors and pump. For the isolated circuit through the pump, set pump rates at 300 mL/h. Optionally, use a second bag of heparinized saline under gravity to provide additional flows for clearing blood out of the pump.
NOTE: Given the prolonged imaging protocol and repeated sampling of the arterial blood, the risk of line occlusion can be high, requiring ongoing vigilance by the investigator team and nurse. Use strict sterility measures and maintain a closed circuit that is configured only by stopcocks.
8. Venous sampling
- In advance of scanning, establish two sites for intravenous access, contralateral to radial artery cannulation for radiopharmaceutical injection, and ipsilateral to radial artery cannulation for venous sampling. Prefer antecubital access.
- In advance of scanning, prepare syringes and syringe caps; indelibly mark syringes and caps, cap all syringes, and weigh capped syringes with an analytical balance to 0.0001 g precision. Record times of venous sampling at the start and completion of drawing at least 2 mL of blood. At room temperature (20-25 °C), centrifuge 1 mL of blood at an RCF of 3,300 × g for at least 60 s to extract plasma. Count activities in whole blood and plasma using a well counter calibrated for 68 Ge.
NOTE: Venous sampling is most appropriate for measurements of [18F]FDG 30-60 min after injection. Venous samples obtained during 15O scanning are technically very challenging and difficult to control and they do not correlate well with arterial samples.
9. PET image reconstruction and data storage
- Reconstruct images from the PET-CT, preferring 3D ordinary-Poisson ordered subsets of expectation maximization (OSEM) with 4-8 iterations of five subsets, TOF, delayed randoms, model-based absolute scatter scaling, attenuation correction, all-pass filtering (no filtering), without point-spread function models, decay correction to start of scanning, rescaling to Bq mL-1, matrix size of 220, zoom 2, and isotropic voxels of 1.65 mm length.
NOTE: Zoom 2 reduces the transverse field of view of image reconstruction by one-half, thereby ignoring ambient space between the participant's head and the PET detector rings. Stated parameters are starting values for [15O]O2 gas, which is highly susceptible to scattering variability, and requires model-based absolute scatter scaling; historically, the choice of models for scattering have strongly impacted the quality of reconstruction of 15O tracers. Furthermore, interactions of vendor-implemented scattering models with other models such as point-spread function models are currently poorly understood. Consequently, this protocol implements only scattering models without point-spread models. - Review reconstructed PET data on the scanner console to ensure adequate radiotracer administration and minimal motion.
- Save DICOM files for reconstructed PET, CT, norms data, and listmode data.
NOTE: Listmode data are essential for optimized reconstructions, which are computationally expensive, and cannot typically be performed at the scanner console. Listmode data are very large (>40 GB per PET session) and adequate storage devices must be reserved.
- Save DICOM files for reconstructed PET, CT, norms data, and listmode data.
10. Discharge and participant follow-up
- Line removal
- Remove the radial arterial catheter using sterile technique and manually apply direct radial artery pressure (this should be done by a qualified healthcare professional).
- Apply pressure for 15 min using the patent hemostasis technique to minimize the risk of radial artery occlusion.
- Inspect the catheter tip for clots or breaks.
- After ensuring that adequate hemostasis has been achieved, apply a pressure dressing with sterile gauze and elastic self-adhesive wrapping. Inspect the hand for any changes in color, temperature, sensation, or function.
- Home-care instructions
- Instruct participants to maintain pressure dressings for 2 h following discharge.
- Instruct the participants to examine the cannulation site for bleeding or bruising at 2 h, and then place over-the-counter bandaging.
- Instruct the participants to avoid bending or wetting the affected wrist/arm for 24 h and avoid strenuous activity involving the wrist/arm for 48 h.
- Instruct the participants to inspect their affected wrist/arm for indications of infection, injury, or bleeding during the 48 h after discharge.
- Provide multiple methods of contacting the study team as needed.
- Provide reassurances for the common complications of mild bruising and transient discomfort.
- Contact the study participant 24-48 h after discharge to ensure that no additional complications have arisen.
- Instruct participants to maintain pressure dressings for 2 h following discharge.
11. Calibrations
- Cross calibration
- Use rod reference sources of 68Ge or 22Na for absolute calibration of well counters.
- Thereafter, cross-calibrate using solutions of 10-37 MBq of [18F]FDG in 30-670 mL of water with 2% acetonitrile or similar organic solvent. Use rigid media bottles (polyethylene terephthalate or high-density polyethylene) that provide radioactivity containment with negligible gamma attenuation. Use smaller-volume bottles to accommodate less activity for cross-calibrating in the scanner bore. Cross-calibrate all other gamma detection instruments using aliquots drawn from the bottle.
- Catheter calibration
- Perform calibration studies of dispersion and delay arising from the use of catheters and lines between the radial artery and the gamma detection probe.
- Use expired blood products from the local blood bank, a controlled temperature bath, and a controlled variation of the hematocrit of blood products.
- Assemble compartmental devices to rapidly alternate between unlabeled and [18F]FDG-labeled blood products, which are delivered to the assembly of catheters, lines, gamma detector probe, and peristaltic pump. Deliver Heaviside "step-function" inputs to the assembly and measure radioactivity over time.
- Estimate the convolution kernel for dispersion and delay. Parameterize kernels to vary with hematocrit. Perform all calibrations with the source of blood products at 37 °C. Reuse the kernel for all human studies employing the identical assembly.
NOTE: These calibrations account only for dispersion and delay through external line assemblies, not internal anatomy.
- Perform calibration studies of dispersion and delay arising from the use of catheters and lines between the radial artery and the gamma detection probe.
Representative Results
Some of the most technically challenging aspects of this protocol involve configuring, managing, and successfully collecting data from arterial lines while simultaneously administering short half-life radiotracers and running the scanner. Figure 1 provides a bird's eye viewpoint of the current setup that summarizes the organization and operational workflows required from study coordinators, interventionalist, nursing, technologists, and investigators. The radiopharmaceuticals described above are easily incorporated into non-quantitative maps of specific activities (Figure 2), including the calculation of ratios of standardized uptake value (SUVR). Whole-brain time activity curves (Figure 3) help identify significant head movements, which would produce discontinuities of the activity curve, and provide characteristic features of tracers, after decay correction, such as the expected plateau of [15O]CO at 120 s and its consequent renal excretion, the plateau of [15O]O2 after bolus passage as it is extracted by brain tissue and metabolized to radiolabeled [15O]H2O, the monotonic decrease of injected [15O]H2O as it increases in volume of distribution throughout the body, and the progressive uptake and phosphorylation of [18F]FDG via hexokinase in the brain over the lifetime of 18F. Detailed model estimates of metabolic [15O]H2O were originally described by Mintun et al15.
A simpler polynomial phenomenology, which omits considerations of intravascular dispersions and emphasizes robust features in emissions data, was advocated by Herscovitch et al26,27. This work's exemplars make use of only this latter phenomenology for oxygen metabolism. Arterial input functions recorded by gamma detection from catheters cannulating the distal radial artery bear substantial dispersion and delay which must be deconvolved. We have favored Bayesian methods for parameter estimation of models of series of gamma distributions and exponentially rising steady terms28. Figure 4 demonstrates results for [15O]CO, [15O]O2, [15O]H2O, and [18F]FDG. Results for [15O]O2 also illustrate the emergence of [15O]H2O of metabolism. Figure 5 demonstrates statistical parameter maps of CBV, CBF, CMRO2, CMRGlc, and AG, which we define to be the molar balance of classical glycolysis: CMRGlc – CMRO2/6.
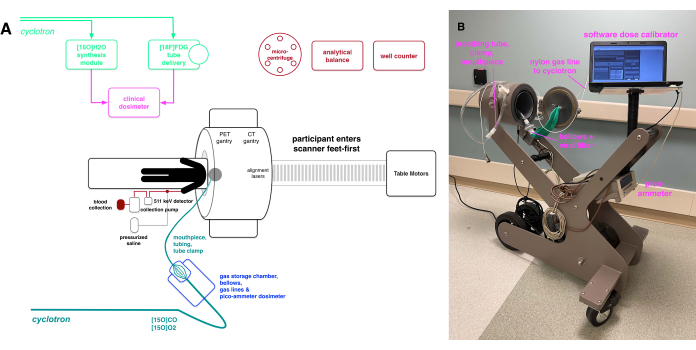
Figure 1: Summary of setup and operational workflows. (A) Schematic illustration of essential instruments and parts needed in the scanner bay. For PET-CT scanners with long scanner bores, feet-first positioning of participants improves the administration of gaseous radiopharmaceuticals by increasing the maneuverability of gas delivery devices and improving verbal and nonverbal communications with the participant. The gas delivery system (cyan and blue) comprises narrow-diameter nylon tubing from the cyclotron, under exhaust for the transport of gaseous radiopharmaceuticals; a shielded gas storage chamber containing expandable bellows and pico-ammeter dose-calibrator; a particulate filter suitable for capturing viral particles; and a terminal large-diameter plastic polymer tubing fitted with clamp and plastic mouthpiece. All parts exposed to respiratory droplets are disposable or compatible with sterilization procedures. Instruments and parts for arterial blood measurements (red and dark gray) provide pressured saline for maintaining radial artery cannulation, compact gamma detection for the coincidence of 511 keV annihilation photons, a peristaltic pump for arterial blood withdrawal, and a container for the collection of withdrawn blood. Radiopharmaceuticals for intravenous injection require synthesis modules for the generation of [15O]H2O from cyclotron-supplied [15O]O2 gas, or pneumatic tube delivery from the cyclotron radiopharmacy (green). Intravenous administration of radiopharmaceuticals requires clinical-grade dosimetry (magenta). Measurements of activity in whole blood and plasma require a well-counter, analytical balance, and microcentrifuge (red). (B) Annotated and detailed views of the gas delivery system. Abbreviation: PET-CT = positron emission tomography-computed tomography. Please click here to view a larger version of this figure.
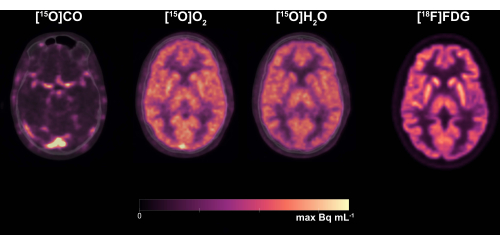
Figure 2: Representative static images for [15O]CO, [15O]O2, [15O]H2O, and [18F]FDG, overlaid with ~25% transparency on CT windowed for temporal bone. Scans of 15O radiotracers positioned the participant feet-first with only elastic self-adhesive wrapping securing the head to the gantry table. The scan of [18F]FDG followed a break from scanning, then returning the participant to approximately the original feet-first positioning. Abbreviations: CO = carbon monoxide; FDG = fludeoxyglucose; CT = computed tomography. Please click here to view a larger version of this figure.
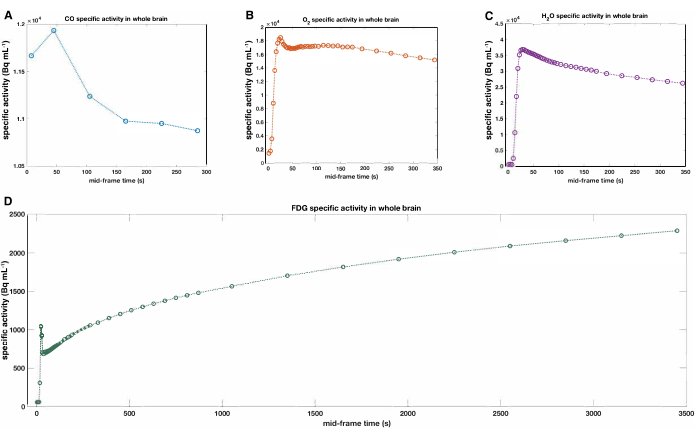
Figure 3: Representative tracer activity curves of the whole brain. (A) [15O]CO, (B) [15O]O2, (C) [15O]H2O, and (D) [18F]FDG. The whole brain was defined by masking of anatomical MPRAGE. The arrival of a bolus of administered tracer precedes or coincides with the timing of the first PET frames in panels A and B. Abbreviations: CO = carbon monoxide; FDG = fludeoxyglucose; PET = positron emission tomography; MPRAGE = magnetization-prepared rapid acquisition gradient echo. Please click here to view a larger version of this figure.
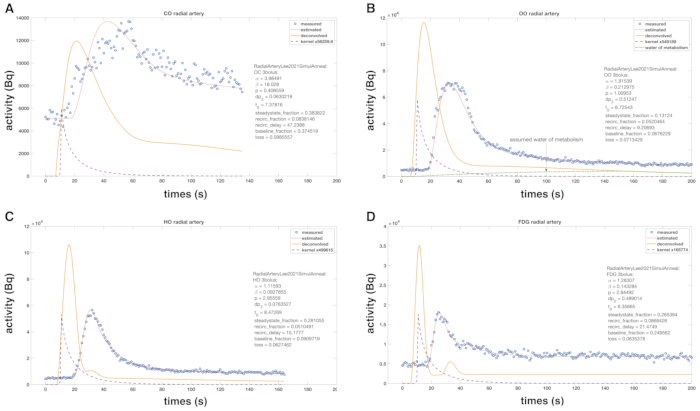
Figure 4: Representative tracer activity curves, continuously sampled from the radial artery and deconvolutions of dispersions and delays in line assemblies. Exemplars describe (A) [15O]CO, (B) [15O]O2, (C) [15O]H2O, and (D) [18F]FDG. Blue circles are data measured by a coincidence detection probe surrounding a narrowly looped catheter that passes arterial blood. Coincidence counting from the probe includes baseline scintillation of LYSO crystals responding to ambient photons (wide spectrum randoms that fall within the device timing window of 100 ns). Arterial blood passes from the radial artery through the probe by distal action of a peristaltic pump. The purple dashed line is the empirical estimate of the kernel for dispersion and delay described in protocol section 11.2. The yellow line describes the tracer activity curve corrected for dispersion and delay. Simulated annealing estimates parameters of a generalized gamma distribution for the yellow line consistent with the estimated kernel and data from coincidence detection. The fitted data appear as a red line. Panel (B) also indicates [15O]H2O from the metabolism of [15O]O2 assumed to have linear characteristics described by Mintun et al.15. Abbreviations: CO = carbon monoxide; FDG = fludeoxyglucose; PET = positron emission tomography; LYSO = lutetium-yttrium oxyorthosilicate. Please click here to view a larger version of this figure.
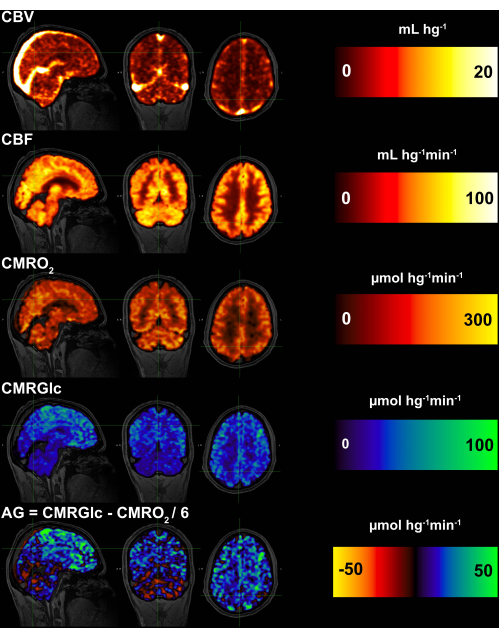
Figure 5: Maps of CBV, CBF, CMRO2, CMRGlc, and AG. CBV is required for the quantitative estimation of CMRO2, CMRGlc, and AG. However, the activity from venous sinuses is confounding for CMRGlc and AG. Consequently, venous sinuses have been removed from CMRO2 and CMRGlc by masking. The contrast between the cerebellum and neocortex is consistent with prior studies of AG. Abbreviations: CBV = cerebral blood volume; CBF = cerebral blood flow; CMRO2 = cerebral metabolic rate of oxygen; CMRGlc = cerebral metabolic rate of glucose; AG = aerobic glycolysis. Please click here to view a larger version of this figure.
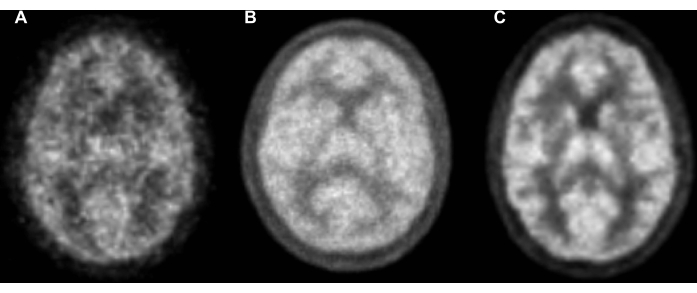
Figure 6: Exemplars of static emissions of [15O]H2O from healthy control study participants scanned on three generations of PET scanners. All reconstructions used 3D OP-OSEM with delayed randoms, attenuation correction, and all-pass filtering (no filtering). All reconstructions are from scanner consoles with parameters suitable for efficient clinical workflows. No additional numerical processing, corrections, or blurring were used. For purposes of comparability, all scanner results are shown following rigid-body transformation and trilinear interpolation to the MNI152 atlas at 1.0 mm3 resolution. (A) A PET-only scanner with BGO crystal scintillators, OP-OSEM with 4 iterations and 16 subsets, 2.0 x 2.0 x 2.4 mm3 voxels, 6 min of emissions, transmission scan with Ge/Ga for attenuation mapping, and single scatter simulations. (B) A PET-MR scanner with LYSO crystal scintillators, OP-OSEM with 4 iterations and 16 subsets, 2.1 x 2.1 x 2.0 mm3 voxels, 10 min of emissions, externally acquired CT for attenuation mapping, and model-based absolute scatter scaling. (C) A PET-CT scanner with LYSO crystal scintillators, time-of-flight detection, OP-OSEM with 8 iterations and 5 subsets, 1.65 x 1.65 x 1.65 mm3 voxels, 6 min of emissions, integrated CT for attenuation mapping, and model-based absolute scatter scaling. Abbreviations: PET = positron emission tomography; CT = computed tomography; MR = magnetic resonance; OP-OSEM = ordinary-Poisson ordered subsets of expectation maximization; BGO = bismuth germanate; LYSO = lutetium-yttrium oxyorthosilicate. Please click here to view a larger version of this figure.
Discussion
PET imaging of oxygen and glucose metabolism using inhaled [15O]CO and [15O]O2 gases, intravenous injection of [15O]H2O, and intravenous injection of [18F]FDG have significant historical priors based on imaging accumulated from older generations of PET scanners14,15,16,17,26,27. These data commonly relied on transmission scanning with germanium/gallium sources for attenuation mapping, luminescence-limited bismuth germanate (BGO) scintillator arrays, high-activity dosing, and 2D acquisitions with ringed septa to accommodate limited scintillator luminescence and filtered back-projection reconstructions that are computationally inexpensive. Newer scanners, including that described in this protocol, use high-resolution CT for attenuation correction, highly luminescent lutetium-yttrium oxyorthosilicate (LYSO) scintillator arrays arranged in spatially dense scintillator configurations, 3D acquisitions that multiplex the efficiency of photon detection, TOF detection electronics that improve spatial localization of annihilation events, and computationally advanced reconstruction methods with 3D ordinary-Poisson ordered subsets of expectation maximization (OP-OSEM). New scanners provide superior image quality at a lower radiation dose29,30. Comparable exemplars from three generations of PET scanners are detailed in Figure 6.
This protocol takes advantage of several additional modifications to advance the quality of information from PET scanning from newer scanners: feet-first positioning, meticulously timed dose administrations, and automated arterial input function measurements25. These permit collection of arterial input functions and brain emissions data for four distinct tracers of oxygen and glucose metabolism within a 2-3 h scanning session. These data can then be submitted to traditional and novel kinetic modeling methods, as well as partial volume correction algorithms, to produce high-resolution, high-accuracy quantitative estimates of brain metabolism. Importantly, this protocol not only permits quantitative measurements of brain oxygen and glucose metabolism but also the calculation of brain AG. Notably, superior image quality from state-of-the-art scanners enables more realistic image-derived arterial input functions as well as novel analytical approaches that were previously limited by noise or sensitivity to timing differences between arterial sampling and brain emissions19.
Notably, imaging quality is more challenging to improve with 15O radiotracers than [18F]FDG. The ephemeral 122 s half-life of 15O causes severe loss of information. However, the use of gaseous radiotracers may also be pertinent, as gases may accumulate in the ambient space between the participant's head and the detection rings of the PET-CT. There, emissions from radiotracer gases can form significant sources of randoms and scattering, thereby confounding vendor-implemented scatter correction methods that use relative scaling of scattering sources compared to regions identified to be air. Even intravenously injected [15O]H2O may pose difficulties if significant amounts are exhaled as [15O]H2O vapor. Methods for scavenging gaseous radiotracers have been reported24 but not implemented in this work. Conventional scatter correction models can be inadequate for imaging 15O radiotracers, and the best performance for these tracers has depended on scattering models that account for the absolute sources of annihilation photons in the field of view, without rescaling, paired with accurate maps of attenuation. Even minor omissions of hardware, such as mirrors attached to head-coils of PET-MR scanners, upon which 15O gases commonly form condensates, can produce substantial artifacts in emissions reconstructions. Related artifacts arising from mismatched maps of attenuation following participant movement have also been reported31. As the interactions of scattering models with point-spread characteristics of gaseous radiotracers are yet poorly characterized, this work has omitted point-spread modeling methods which otherwise are essential for high-resolution PET. Optimizing reconstruction parameters for listmode for each tracer is best practice, but this work provides exemplars using simply console reconstructions that were identically applied to all tracers, as possible, as described in protocol section 9.1. Exemplars necessarily demonstrate frame timing schedules that have been adapted to the variability of tracer-kinetic timescales. The exemplars emphasize simplicity, comparability of counting statistics, and effective spatial resolutions available for each tracer, and minimizing bias that could arise while optimizing reconstruction parameters for each tracer. For comparability with existing studies of 15O, the representative results of this work use 8 iterations of 5 subsets, previously reported to be appropriate for modern PET-CT with time-of-flight acquisitions30,32. Time-of-flight may yield improved imaging resolution with 4 iterations of 5 subsets, and these optimizations are under active investigation for the tracers described in this work.
The longer scanner bore of modern PET-CT scanners encumbers investigators providing radiotracer gases. Confined gantry geometries increase the difficulties of reaching the participant's mouth when administering gases, communicating instructions to participants, and ensuring that gas administration devices do not leak radiotracers into the ambient space. Thereby, feet-first positioning of participants demonstrates advantages. Most scanner hardware makes feet-first positioning incompatible with the placement of neuroshielding devices, which typically place lead shielding that surrounds the participant's neck and partitions the participant's head from the body. Neuroshielding will reduce randoms entering the field-of-view from the body. The relative benefits of neuroshielding compared to avoidance of ambient gas radiotracers are presently poorly understood.
Quantifying brain metabolism
This paper demonstrates the results of analyses using traditional models for hemodynamics described by Raichle et al. (CBF)16 and Martin et al. (CBV)17, and for metabolism described by Mintun et al. (CMRO2)15 and Huang et al. (CMRGlc)14. These analyses utilize the arterial input functions and emissions data measured using the protocol described in this paper. Alternative means to measure the arterial input function, such as an image-derived method, are being actively pursued and tested against the invasive method. Traditional models also make full use of dynamic imaging to estimate kinetic model parameters. We have preferred the use of polynomial representations of CBF and CMRO226,27. We have favored the methods of Huang et al. for estimating CMRGlc but employing Bayesian parameter estimation28,33. AG was more recently conceived as a measure of glucose that enters glycolytic pathways but contributes to cellular functions other than oxidative phosphorylation4. Calculation of brain AG then simply requires conversion of CMRGlc and CMRO2 to molar equivalents and subtraction of one-sixth of the latter from the former.
Partial volume correction
We commonly perform regional partial volume correction on SUVR images using the symmetric geometric transfer matrix algorithm (sGTM)34. This relies on the high-resolution data obtained by MRI, which can include anatomic sequences alone, though the current protocol also obtains Human Connectome Project (HCP)-like sequences for more precise regional parcellation. We have used both anatomic (e.g., Desikan-Killiany35) and functional (e.g., Schaeffer36 or Glasser37) atlases. The former atlases often have larger regions of interest that are more appropriate for PET images obtained at a lower resolution and have been more widely used in prior PET research. However, the newer atlases are functionally and cytoarchitecturally more well-defined and may now be more applicable with higher-resolution PET imaging, such as that obtained with the Siemens Vision scanner. SUVR images for 15O scans are calculated as have been previously described and referenced to whole brain values4. Whole-brain CMRGlc and CMRO2 are then calculated using the kinetic modeling as per above to convert the SUVR images to absolute quantitative values. From this, partial volume corrected regional AG can then be calculated. While our exemplars for dynamic emissions imaging do not demonstrate partial volume correction for simplicity of presentation, partial volume correction methods that account for dynamic imaging are now being actively investigated.
Generalizability and adaptability of the protocol
This protocol describes methodological details pertinent to acquiring the highest achievable accuracy, precision, reproducibility, and interpretability from measurements of oxygen and glucose metabolism by PET in humans. The highest known accuracy and precision of measurements belong to analyses based upon principles and practices of tracer kinetics, which include direct measurements of arterial input functions, determination of regions of interest by co-registration with high-resolution structural MRI, and highly demanding use of computational resources for statistical models. In particular, invasive radial-artery cannulation, and its maintenance over serially repeated emission scans, is costly and bears finite risks of serious injury that demand the involvement of clinically experienced teams. The use of tracers based on 15O is yet another challenge for cyclotrons and their support teams. These provide correspondence with historically reported metabolic measurements in humans and ensure that interpretations of quantitative findings are built upon prior accumulated information. However, these detailed and invasive measures also provide means for validation of less invasive, less demanding methods that may be sufficient for many questions of human metabolism. Following appropriate validation, radial artery cannulation may be suitably replaced with image-derived sources of input functions38 for many specialized studies. Avoiding radial artery cannulation also precludes direct measurements of the primary metabolic product of [15O]O2, namely [15O]H2O, which can be estimated from samples of radial artery that have been centrifuged to estimate [15O]H2O of metabolism from plasma and [15O]O2 from centrifuged red blood cells. However, computationally intensive methods can be used to parametrically solve for the emergence of metabolic [15O]H2O in the arterial circulation, a linear model of which has been proposed by Mintun et al15. Many methodologies using SUVR may also be amenable to validation following comparisons to invasively obtained data. Currently, active research programs seek validation of oxygenation estimates based on the blood oxygenation level-dependent effect, and contemporaneous measurements with 15O can provide further validation39. Additionally, while only mentioned in this protocol without exemplars, detailed optimizations of image reconstructions from listmode are likely to improve the quality of measurements of metabolism. Further, many specialized methods such as motion correction of listmode data and partial volume corrections, may merit effort when study questions demand them, for example, when occasional participants have excessive head movements or studies of cortical atrophy are confounded by partial volume averaging with cerebral spinal fluid.
Cautions for PET scanning
This protocol exposes participants to ionizing gamma radiation. The current estimates of radiation in participants who have undergone the total PET session described here (including four to six 15O scans and one FDG scan), result in an average total effective dose, inclusive of all radiotracer administrations, of approximately 7 mSv (0.7 rem). This is comparable to the radiation dose of other radiotracers used in research and clinical practice and represents 14% of the total radiation dose allowable to a radiation worker in one year. All participants (and/or their legally acceptable representative) are carefully informed both in writing and verbally of the potential radiation risks prior to obtaining their consent for study enrollment.
Cautions for arterial lines
Complications of arterial cannulation include bruising (common), pain, swelling, hematoma (uncommon), bleeding at the site of insertion, vasospasm, thrombosis (rare), and reaction to heparinized saline when used (very rare). We routinely employ an interventional radiology service to place arterial lines and manage any complications if they should arise.
Cautions for MRI
The US Food and Drug Administration requires all medical devices that enter the magnetic field of an MRI scanner to undergo standardized safety testing. If a participant's device is labeled MRI Safe, then we can proceed using standard FDA-approved scanning conditions without additional risks to the participant. If a participant's device is MRI Conditional, we review the manufacturer, make, and model of the device, and then adjust the MRI scanning procedures accordingly. Imaging also has the potential risk of revealing incidental findings, which can incur additional risks such as anxiety, financial loss from additional work-up, and, rarely, complications arising from subsequent, clinically indicated invasive procedures.
Summary of limitations
Unavoidable limitations of measuring oxygen and glucose metabolism are specific to the radiotracer themselves. 15O-tracers have short half-lives that stipulate many of the most demanding requirements of this protocol, including the presence of highly specialized and accessible cyclotron facilities. Gaseous 15O-tracers introduce the complexity of gas management such as scavenging of expired gases24 and specialized methods for scatter corrections. [18F]FDG exchanges the considerable challenges of tracking metabolites in [11C]-glucose tracers for confounding by lumped-constant estimations. This protocol also has limitations arising from the confining geometry of integrated PET-CT scanners. While feet-first positioning of the participant ameliorates confinement problems, it may be incompatible with the use of neuroshielding devices. Finally, the use of invasive radial artery cannulation is itself a significant limitation. The radial artery is a proxy for the primary arterial supply of the brain. However, the radial artery may have discrepant flow characteristics from arterial supplies to the brain. Furthermore, invasive and painful procedures alter the cognitive state of study participants, limiting the scope and generalizability of neuroimaging studies that can be pursued by this protocol.
Divulgations
The authors have nothing to disclose.
Acknowledgements
We are particularly grateful to our research participants for their altruism. We acknowledge the directors and staff of the Neuroimaging Labs Research Center, Knight Alzheimer's Disease Research Center, Center for Clinical Imaging Research (CCIR), and the Washington University cyclotron facility for making this research possible. We gratefully acknowledge research funding from NIH R01AG053503, R01AG057536, RF1AG073210, RF1AG074992, and 1S10OD025214, the Mallinckrodt Institute of Radiology, and the McDonnell Foundation for Systems Neuroscience at Washington University.
Materials
| 3/16" outer diameter 1/8" innner diameter nylaflow tubing | Nylaflow Tubing, Zazareth, PA | ||
| 4 x 4 in. gauze | McKesson MedSurg | 16-4242 | |
| Analytical balance | Fisher Scientific/OHUAS | Pioneer Exal Model 90 mm platform #PA84 | |
| Bacterial/Viral filter | Hudson RCI, Teleflex, Perak, Malaysia | REF 1605 (IPN042652) | |
| BD SmartSite Needle-Free Valve | Becton Dickinson | 2000E | |
| Biograph mMR | Siemens, Erlangen, Germany | ||
| Biograph Vision 600 Edge | Siemens, Erlangen, Germany | ||
| Caprac wipe counter | Mirion Medical (Capintec), Florham Park, NJ | from 1991 or newer | NaI drilled well crystal |
| Coban self-adhesive wrap | 3M | commonly used in intensive care units | |
| dressing, tegaderm, 4 x 4" | 3M Health Care | #1626 | |
| ECAT EXACT HR+ | CTI PET Systems, Knoxville, TN | ||
| Edwards TruWave 3 cc/84 in (210 cm) | Edwards Lifescience | PX284R | |
| extension catheter 48 cm length, 0.642 mL priming volume | Braun | V5424 | |
| heparin sodium, solution 2 U/mL, 1,000 mL | Hospira Worldwide | #409762059 | |
| I.V. armboard flexible 4 x 9 in. adult | DeRoyal | M8125-A | |
| Keithley pico-ammeter | Tekronix | ||
| Magnetom Prisma fit | Siemens, Erlangen, Germany | 3T | |
| male-male adapter for Luer valves | Argon Medical Co. | 040184000A | |
| MiniSpin Personal Microcentrifuge | Eppendorf, Hamburg, Germany | EP-022620151 | |
| Mouthpiece 15 mm ID, 22 mm OD | Hudson RCI, Teleflex, Perak, Malaysia | REF 1565 (IPN042595) | |
| MRIdium | Iradmed, Winter Springs, FL | 3860+ | |
| Nalgene square PET media bottle with closure, 650 mL | Thermo Scientific | #3420400650 | for cross-calibration |
| pressure infusion bag with bulb, accommodating 1,000 mL | Health Care Logi | #10401 | |
| pressure monitoring tray polyethylene catheter; 2.5Fr (2.5 cm) angiocath; 0.015" 15 cm wire; 22G (2 cm) needle | Cook Medical | C-P MSY-250, G02854 | |
| RDS 11 MeV Cyclotron | Siemens, Erlangen, Germany | proton bombardment of 15N to generate 15O | |
| sodium chloride IV solution 0.9%, 1,000 mL | B. Braun Medical | E8000 | |
| steri-strips (closure, skin reinf LF 1/2×4") | McKesson MecSurg | #3010 | |
| Twilite II | Swisstrace, Zurich, Switzerland | ||
| Uninterruptible Power Supply battery backup and surge protector | APC | BR1500MS2 |
References
- Goyal, M. S., Hawrylycz, M., Miller, J. A., Snyder, A. Z., Raichle, M. E. Aerobic glycolysis in the human brain is associated with development and neotenous gene expression. Cell Metabolism. 19 (1), 49-57 (2014).
- Magistretti, P. J. Imaging brain aerobic glycolysis as a marker of synaptic plasticity. Proceedings of the National Academy of Sciences. 113 (26), 7015-7016 (2016).
- Shannon, B. J., et al. Brain aerobic glycolysis and motor adaptation learning. Proceedings of the National Academy of Sciences of the United States of America. 113 (26), E3782-E3791 (2016).
- Vaishnavi, S. N., et al. Regional aerobic glycolysis in the human brain. Proceedings of the National Academy of Sciences. 107 (41), 17757-17762 (2010).
- Powers, W. J., Dagogo-Jack, S., Markham, J., Larson, K. B., Dence, C. S. Cerebral transport and metabolism of 1-11C-D-glucose during stepped hypoglycemia. Annals of Neurology. 38 (4), 599-609 (1995).
- Locasale, J. W., Cantley, L. C. Metabolic flux and the regulation of mammalian cell growth. Cell Metabolism. 14 (4), 443-451 (2011).
- Lunt, S. Y., Vander Heiden, M. G. Aerobic glycolysis: meeting the metabolic requirements of cell proliferation. Annual Review of Cell and Developmental Biology. 27 (1), 441-464 (2011).
- Vlassenko, A. G., Raichle, M. E. Brain aerobic glycolysis functions and Alzheimer’s disease. Clinical and Translational Imaging. 3 (1), 27-37 (2015).
- Goyal, M. S., et al. Loss of brain aerobic glycolysis in normal human aging. Cell Metabolism. 26 (2), 353-360 (2017).
- Goyal, M. S., et al. Spatiotemporal relationship between subthreshold amyloid accumulation and aerobic glycolysis in the human brain. Neurobiology of Aging. 96, 165-175 (2020).
- Goyal, M. S., et al. Brain aerobic glycolysis and resilience in Alzheimer disease. Proceedings of the National Academy of Sciences of the United States of America. 120 (7), 2212256120 (2023).
- Segarra-Mondejar, M., et al. Synaptic activity-induced glycolysis facilitates membrane lipid provision and neurite outgrowth. EMBO Journal. 37 (9), 97368 (2018).
- Harris, R. A., et al. Aerobic glycolysis is required for spatial memory acquisition but not memory retrieval in mice. Eneuro. 6 (1), (2019).
- Huang, S. C., et al. Noninvasive determination of local cerebral metabolic rate of glucose in man. American Journal of Physiology-Endocrinology and Metabolism. 238 (1), E69-E82 (1980).
- Mintun, M. A., Raichle, M. E., Martin, W. R. W., Herscovitch, P. Brain oxygen utilization measured with O-15 radiotracers and positron emission tomography. Journal of Nuclear Medicine. 25 (2), 177-187 (1984).
- Raichle, M. E., Martin, W. R., Herscovitch, P., Mintun, M. A., Markham, J. Brain blood flow measured with intravenous H2(15)O. II. Implementation and validation. Journal of nuclear medicine. 32 (15), 790-798 (1983).
- Martin, W. R. W., Powers, W. J., Raichle, M. E. Cerebral blood volume measured with inhaled C15O and positron emission tomography. Journal of Cerebral Blood Flow & Metabolism. 7 (4), 421-426 (1987).
- Hooker, J. M., Carson, R. E. Human positron emission tomography neuroimaging. Annual Review of Biomedical Engineering. 21, 551-581 (2019).
- Fan, A. P., et al. Quantification of brain oxygen extraction and metabolism with [(15)O]-gas PET: A technical review in the era of PET/MRI. Neuroimage. 220, 117136 (2020).
- Tisdall, M. D., et al. Volumetric navigators for prospective motion correction and selective reacquisition in neuroanatomical MRI. Magnetic Resonance in Medicine. 68 (2), 389-399 (2012).
- Greve, D. N., et al. Cortical surface-based analysis reduces bias and variance in kinetic modeling of brain PET data. NeuroImage. 92, 225-236 (2014).
- Greve, D. N., et al. Different partial volume correction methods lead to different conclusions: An 18F-FDG-PET study of aging. NeuroImage. 132, 334-343 (2016).
- Iguchi, S., et al. System evaluation of automated production and inhalation of (15)O-labeled gaseous radiopharmaceuticals for the rapid (15)O-oxygen PET examinations. EJNMMI Physics. 5 (15), 37 (2018).
- Alf, M. F., et al. Quantification of brain glucose metabolism by 18F-FDG PET with real-time arterial and image-derived input function in mice. Journal of Nuclear Medicine. 54 (1), 132-138 (2013).
- Herscovitch, P., Mintun, M. A., Raichle, M. E. Brain oxygen utilization measured with oxygen-15 radiotracers and positron emission tomography: generation of metabolic images. Journal of Nuclear Medicine. 26, 416-417 (1985).
- Videen, T. O., Perlmutter, J. S., Herscovitch, P., Raichle, M. E. Brain blood volume, flow, and oxygen utilization Measured with 15O radiotracers and positron emission tomography: revised metabolic computations. Journal of Cerebral Blood Flow & Metabolism. 7 (4), 513-516 (1987).
- Lee, J. J., et al. Dynamic susceptibility contrast MRI with localized arterial input functions. Magnetic Resonance in Medicine. 63 (5), 1305-1314 (2010).
- Kunnen, B., Beijst, C., Lam, M., Viergever, M. A., de Jong, H. Comparison of the Biograph Vision and Biograph mCT for quantitative (90)Y PET/CT imaging for radioembolisation. EJNMMI Physics. 7 (1), 14 (2020).
- van Sluis, J., et al. Performance characteristics of the digital Biograph Vision PET/CT system. Journal of Nuclear Medicine. 60 (7), 1031-1036 (2019).
- Lodge, M. A., Mhlanga, J. C., Cho, S. Y., Wahl, R. L. Effect of patient arm motion in whole-body PET/CT. Journal of Nuclear Medicine. 52 (12), 1891-1897 (2011).
- Prenosil, G. A., et al. Performance characteristics of the Biograph Vision Quadra PET/CT system with a long axial field of view using the NEMA NU 2-2018 Standard. Journal of Nuclear Medicine. 63 (3), 476-484 (2022).
- Lee, J. J., et al. Dissociation between hormonal counterregulatory responses and cerebral glucose metabolism during hypoglycemia. Diabetes. 66 (12), 2964-2972 (2017).
- Sattarivand, M., Kusano, M., Poon, I., Caldwell, C. Symmetric geometric transfer matrix partial volume correction for PET imaging: principle, validation and robustness. Physics in Medicine and Biology. 57 (21), 7101-7116 (2012).
- Desikan, R. S., et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 31 (3), 968-980 (2006).
- Schaefer, A., et al. Local-global parcellation of the human cerebral cortex from intrinsic functional connectivity MRI. Cerebral Cortex. 28 (9), 3095-3114 (2018).
- Glasser, M. F., et al. A multi-modal parcellation of human cerebral cortex. Nature. 536 (7615), 171-178 (2016).
- Zanotti-Fregonara, P., Chen, K., Liow, J. -. S., Fujita, M., Innis, R. B. Image-derived input function for brain PET studies: many challenges and few opportunities. Journal of Cerebral Blood Flow & Metabolism. 31 (10), 1986-1998 (2011).
- Rodgers, Z. B., Detre, J. A., Wehrli, F. W. MRI-based methods for quantification of the cerebral metabolic rate of oxygen. Journal of Cerebral Blood Flow & Metabolism. 36 (7), 1165-1185 (2016).

.