All research was performed in compliance with institutional guidelines for the care of animals.
1. Considerations and preparations for the experiment
- Utilize a suitable pulse duplicator (PD) for the simulation of cardiac output through the AV. The PD will need to be able to accommodate biological materials and be able to be cleaned.
- Utilize PD settings appropriate for testing the AV: 70 mL displacement volume and 70 beats per minute (5 L/min cardiac output), 35% of the cardiac cycle in systole, 100 mmHg mean transvalvular pressure gradient, 120 maximum pressure gradient, and 80 minimum pressure gradient.
- Use room temperature (RT) normal saline (0.9% NaCl) as the fluid medium.
- Locate or create (using 3D printing or a similar method) suitable fixtures for mounting the porcine AV for testing on the PD.
- Utilize fixtures that are modeled on the fixtures provided with the pulse duplicator with the following specifications: ensure that the inner diameter of the fixture is similar to the diameter of the AV being studied, the attachment length is at least 2 cm, and the usable attachment width is at least 4 cm (Figure 1).
- Use rubber O-rings as gaskets on the ends of the fixtures.
- Obtain a heart specimen after cardiectomy (Figure 2A).
- Use porcine cardiac specimens from the slaughterhouse or waste tissue from animals that are otherwise healthy and have not been part of any experimental protocols that will affect their hearts.
- Obtain specimen after cardiectomy or perform post-mortem cardiectomy, including transection of the superior vena cava, inferior vena cava, main pulmonary artery (PA), all pulmonary veins, and aorta at the distal aspect of the aortic arch.
NOTE: Fresh specimens, less than 6 h post-mortem or stored in sterile saline with a 1% antibiotic solution (penicillin and streptomycin) in a 4 oC refrigerator for up to 7 days, should be used for this experiment. Tissues fixed in formalin or glutaraldehyde will produce altered hydrodynamic results due to increased stiffness.
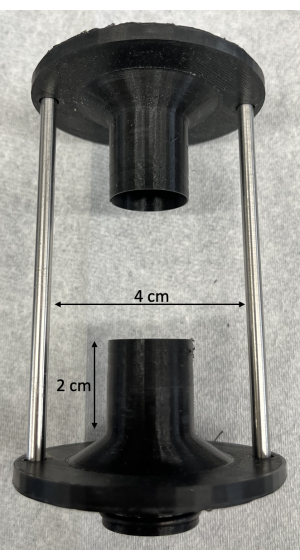
Figure 1: Custom 3D printed fixtures for mounting the porcine aortic valves on the pulse duplicator. As noted in the protocol, the attachment length should be at least 2 cm, and the usable attachment width should be at least 4 cm. Please click here to view a larger version of this figure.
2. Resection of right-sided structures
- Dissect the PA off the aorta with Metzenbaum scissors until ventricular tissue is visible (Figure 2B).
- Dissect and ligate with silk ties both coronary arteries at their origin from the aortic sinuses, taking care not to narrow the sinuses.
- Transect the coronary arteries distal to the silk ties.
- Incise the right ventricle (RV) between the aorta and the PA at the base of the pulmonary valve using Metzenbaum scissors (Figure 2C).
- Beginning anteriorly, continue the incision circumferentially along the interventricular septum to remove the RV free wall (Figure 2D, E).
- Continue the incision posteriorly through the tricuspid valve annulus along the interatrial septum to remove all right atrial tissue (Figure 2F).
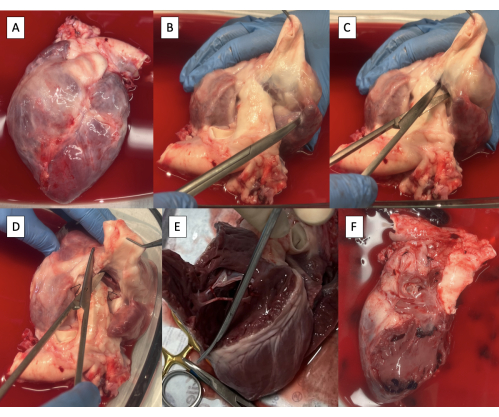
Figure 2: Cardiectomy specimen and resection of right-sided structures. (A) Cardiectomy specimen. (B) Main pulmonary artery dissected off the aorta until ventricular tissue is visible. (C) Incising the right ventricle (RV) at the base of the pulmonary valve. (D) Continuing the incision along the interventricular septum anteriorly. (E) Removing the RV-free wall by continuing the incision circumferentially along the interventricular septum. (F) Specimen with right-sided structures removed. Please click here to view a larger version of this figure.
3. Preparation of the left ventricular outflow tract (LVOT) for cannulation with the PD fixture
- Incise the left atrium (LA) through the right pulmonary vein ostium parallel to the aorta using Metzenbaum scissors (Figure 3A).
NOTE: Although limited variability exists, porcine pulmonary vein anatomy generally terminates in two pulmonary vein ostia entering the LA8. - Continue the incision towards the anterolateral commissure of the mitral valve (MV), leaving at least a 3 mm cuff of atrial tissue on the aorta side.
- Trim excess LA tissue, maintaining the 3 mm cuff of atrial tissue on the aorta and the MV annulus circumferentially (Figure 3B).
- Extend the incision onto the left ventricle (LV) through the anterolateral commissure of the MV, taking care to preserve the anterolateral papillary muscle (Figure 3C).
- Divide chordae tendineae from the anterolateral papillary muscle to the posterior MV leaflet, preserving attachments to the anterior MV leaflet.
- Continue the incision to the apex of the heart.
- Trim excess LV tissue below the papillary muscles, preserving both papillary muscles (Figure 3D).
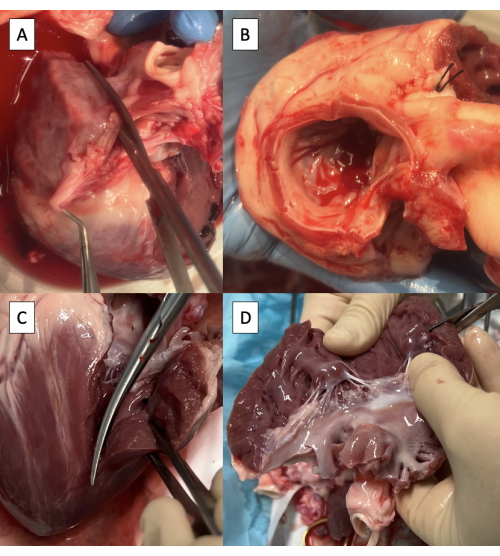
Figure 3: Preparation of the left ventricular outflow tract for cannulation with the pulse duplicator fixture. (A) Incising the left atrium (LA) through the ostium of the right pulmonary vein. (B) Excess LA tissue trimmed, maintaining at least a 3 mm cuff of atrial tissue on the aorta and maintaining the mitral valve annulus circumferentially. (C) Extending the incision onto the left ventricle (LV) through the anterolateral commissure of the mitral valve. (D) Removing excess LV tissue below the papillary muscles. Scissors are visible in the upper right corner of the image. Please click here to view a larger version of this figure.
4. Preparation of the aorta for cannulation with the PD fixture
- Trim any excess lymphatic, connective, or pulmonary artery tissue off the aorta (Figure 4A).
- Incise the superior aspect of the aortic arch from the descending aorta to the left subclavian artery using Metzenbaum scissors (Figure 4B).
- Continue the incision on the superior aspect of the aortic arch from the left subclavian artery to the brachiocephalic trunk (Figure 4C, D).
NOTE: Branches of the porcine aortic arch from distal to proximal include the left subclavian artery and the brachiocephalic trunk, which gives rise to the right subclavian artery, right carotid artery, and left carotid artery9.
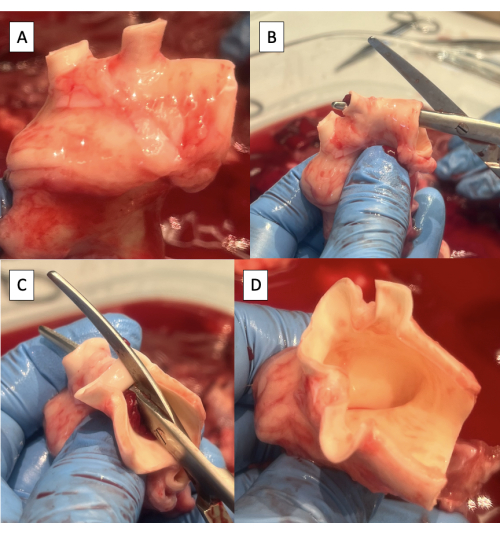
Figure 4: Preparation of the aorta for cannulation with the pulse duplicator fixture. (A) Aortic arch with excess tissue removed. Note the two arch vessels in the porcine aortic arch, the brachiocephalic trunk, and the left subclavian artery. (B) Starting the incision along the superior aspect of the aortic arch from the descending aorta to the left subclavian artery. (C) Continuing the incision along the superior aspect of the aortic arch from the left subclavian artery to the brachiocephalic trunk. (D) Completed aortic arch incision. Please click here to view a larger version of this figure.
5. Cannulation of the LVOT with the PD fixture
- Test the positioning of the fixture in the LVOT and trim excess LV tissue.
- Insert the fixture into the LVOT under the anterior leaflet of the MV.
- Wrap the LV-free wall around the fixture.
- Trim excess LV tissue to maintain a tight wrap around the fixture.
- Remove half of the thickness of the LV free wall starting at the interventricular septum, maintaining at least 1 cm of epicardium at the free edge to maintain the integrity of the suture line (Figure 5A).
- Trim 1 cm of tissue off the superior corner of the LV free wall wrap (Figure 5A).
- Position the fixture in the LVOT with the supporting rod attachment hole 1 cm behind the LV incision (Figure 5B).
- Take care not to insert the fixture too far into the LVOT such that it dilates the AV annulus.
- Fasten the anterior leaflet of the MV to the fixture using one or two 6-inch zip ties positioned between the chordae tendineae of the leaflet (Figure 5C).
- Suture the LV free wall around the fixture (Figure 5D).
- Start by suturing the cuff of LA tissue on the aorta to the MV annulus using a simple running suture with a taper point needle.
- Continue the running stitch onto the LV, not tearing the LV tissue.
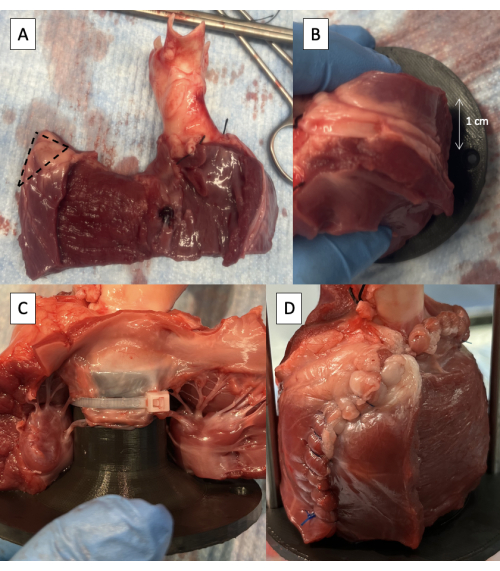
Figure 5: Cannulation of the left ventricular outflow tract with the pulse duplicator fixture. (A) One-half thickness of the LV free wall removed with 1 cm of epicardium maintained at the free edge. The dotted line indicates the 1 cm area to be removed from the superior corner of the LV free wall wrap. (B) Supporting rod attachment hole positioned 1 cm behind the LV free wall incision. (C) Zip tie fastening the anterior leaflet of the MV to the proximal fixture. (D) LV free wall sutured around the fixture. Please click here to view a larger version of this figure.
6. Cannulation of the aorta with PD fixture and final preparation for PD testing
- Measure the diameter of the AV using Hegar dilators to assist with the interpretation of the results of PD testing.
- Identify the neutral position of the aorta by lifting the specimen off the table by grasping the aorta (Figure 6A).
- Insert the PD fixture into the aorta, taking care to line up the rod attachment holes in the neutral position of the aorta.
- Check the length of the specimen by inserting the support rods.
- Secure the PD fixture to the aorta using one or two 6-inch zip ties (Figure 6B).
- Secure the LVOT around the PD fixture using one or two 8-inch zip ties.
- Secure the support rods in place using screws provided with the PD set.
- Place the specimen in PD and start the test (Figure 6C, Video 1, and Video 2).
- Suture any leaks as needed.
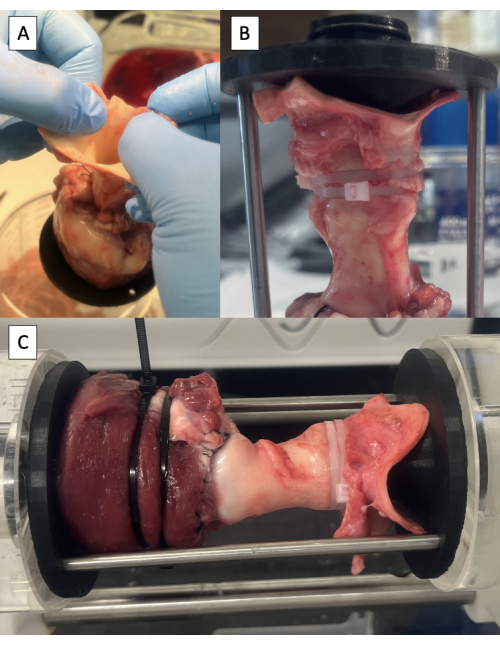
Figure 6: Cannulation of the aorta and testing in the pulse duplicator. (A) Lifting the specimen off the table by the aorta to identify the neutral position of the aorta. (B) Distal fixture secured in the aorta with zip ties. (C) Specimen mounted in the pulse duplicator for hydrodynamic testing. Please click here to view a larger version of this figure.
7. Perform experimental procedure
NOTE: Perform experimental procedures like, the Ozaki procedure as previously described5,6,7, and repeat PD testing.
- If the tissue has become desiccated during the procedure, tighten the zip ties and reinforce the suture line as needed.
8. Long-term storage of specimen (if desired)
- Place specimen in formalin 10% for 168 h (1 week)10,11.
- After tissue fixation, wash the specimen with deionized water and place it in ethanol 70% for long-term storage.
