In this study, 24 patients were enrolled presenting with upper limb dysfunction combined with various types of cognitive impairment following a stroke. The observed types of cognitive impairment included Amnesia, Agnosia, Executive Dysfunction, Attentional Impairments, among others. No statistically significant differences were found between the two groups in terms of sex, age, duration of disease, and type of stroke (P > 0.05), as detailed in Table 1. The experimental group, which underwent upper limb rehabilitation using the digital occupational training system, exhibited greater improvements in FMA-UE14, MoCA13, and MBI17 compared to conventional therapy (Table 2).
Following the training period, the experimental group demonstrated a significant improvement in MoCA scores (P < 0.05), while the control group did not show significant differences (P > 0.05). Moreover, the improvement in the experimental group was more pronounced than in the control group (P < 0.05) (Table 2). Regarding FMA upper limb scores, the experimental group showed significant improvement after 8 weeks of training (P < 0.05), with a notable difference in improvement compared to the control group (P < 0.05) (Table 2). Concerning BI scores, both groups exhibited significant improvements compared to before the intervention (P < 0.05), and the improvement in the experimental group was significantly different from that in the control group (P < 0.05) (Table 2). These findings underscore the effectiveness of the digital occupational training system in enhancing patients' cognitive and upper limb abilities, surpassing traditional rehabilitation therapy in cognitive improvements.
Statistical analyses were conducted using a statistical software (see Table of Materials), with the significance level set at a two-tailed P < 0.05. Parametric analysis, assuming data normality and homogeneity of variance, employed the independent samples t-test to compare differences between groups in scale scores.

Figure 1: Digital Occupational Training System. The system's screen is positioned at an ergonomically suitable height and angle for stroke patients in a seated or standing position, promoting interactive engagement for rehabilitation exercises. Please click here to view a larger version of this figure.
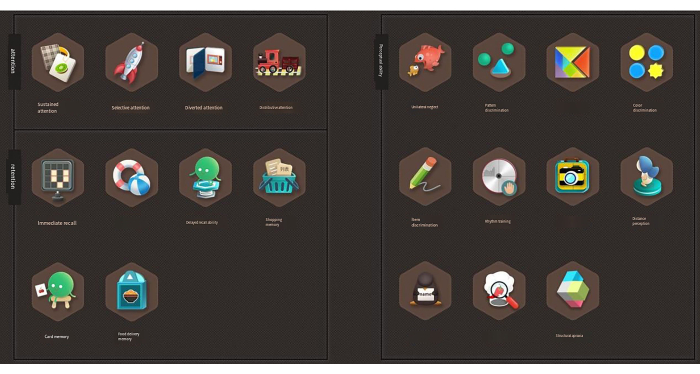
Figure 2: Game content and application of cognitive-based upper limb VR scheme. This figure graphically illustrates various tasks within the game, each meticulously designed to target specific cognitive and motor skills. Please click here to view a larger version of this figure.
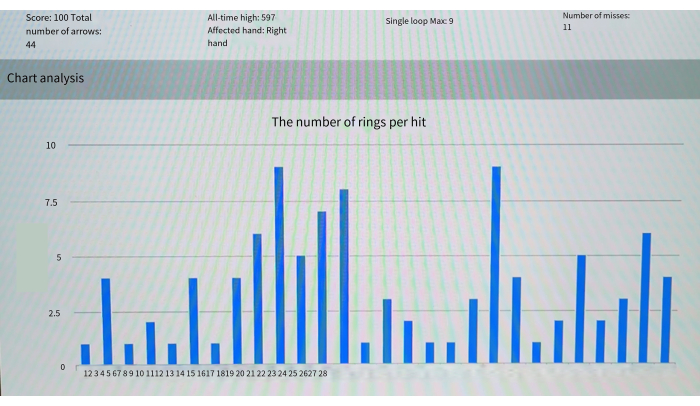
Figure 3: Analysis of archery game training results – the number of rings per target hit. This figure provides a statistical breakdown of participants' performances within the archery game, visualizing the number of rings hit per target across multiple sessions. Please click here to view a larger version of this figure.
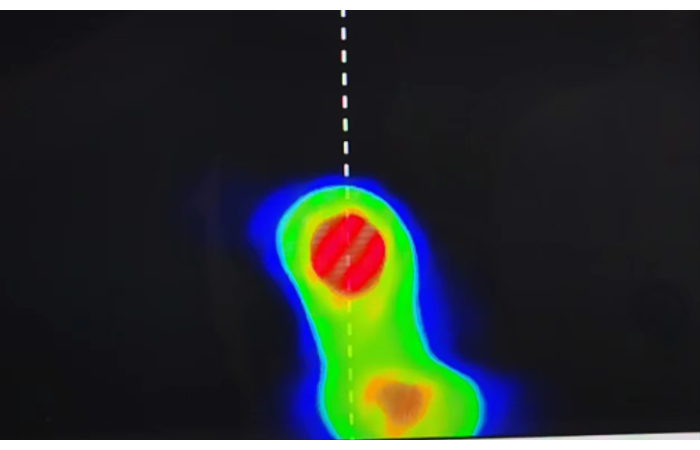
Figure 4: Analysis of archery game training results map of active areas. The color gradients represent areas of high and low activity, providing insight into the accuracy and focal points of participants' attempts, thus serving as a visual tool to assess motor control and coordination throughout the training. Please click here to view a larger version of this figure.
| Group | n | Sex (n) | Age (x±s, y ) | Course of the disease (x±s, d) | Type of stroke (n) | Hemiplegic side (n) | |||||
| Male | Female | Ischemic | Hemorrhagic | Left | Right | ||||||
| Control group (n = 12) | 12 | 6 | 6 | 50.50 ± 5.50 | 37.08 ± 11.48 | 7 | 5 | 7 | 5 | ||
| Experimental group (n = 12) | 12 | 7 | 5 | 50.42 ± 5.52 | 36.0 ± 10.86 | 8 | 4 | 6 | 6 | ||
| P | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 | ||||||
Table 1. Baseline characteristics between the two groups. It presents a comprehensive comparison of baseline characteristics between the control and experimental groups. This includes demographic and clinical data, ensuring comparability between the groups and verifying the randomization process, hence confirming the robustness of the subsequent analysis.
| Group | MoCA | FMA-UE | MBI | |
| Control group (n = 12) | Per-treatment | 18.25 ± 2.42 | 31.83 ± 6.26 | 57.42 ± 7.37 |
| Post-treatment | 19.0 ± 3.16 | 35.58 ± 5.04 | 64.33 ± 6.51 * | |
| Experimental group (n = 12) | Per-treatment | 18.33 ± 2.34 | 32.42 ± 5.84 | 57.33 ± 9.50 |
| Post-treatment | 22.00 ± 2.92 **# | 40.67 ± 6.72**# | 71.42 ± 9.63 **# | |
| *P < 0.05, compared to pre-treatment; #P < 0.05, compared to the control group | ||||
Table 2. Comparison of MoCA, FMA-UE, and MBI scores between two groups before and after training (x ± s). *P < 0.05, compared to pre-treatment. #P < 0.05, compared to the control group. The statistically significant values are highlighted, elucidating the impact of the VR-based training regime on cognitive and motor functions and showcasing the relevant improvements in participants' capabilities post-training.
