The outlined protocol was designed for easy reproducibility in clinical practice. Minimal modifications were made to the available module for Normothermic Ex-situ Heart Perfusion (NESP). The only adjustments were made to connect the module to an extracorporeal life support pump, an oxygenator, and a heater-cooler unit to replace the machine perfusion (MP).
Two test procedures were initially conducted to assess the coronary angiography views used in this protocol. Six coronary angiographies were then performed on ex-situ perfused porcine hearts. Hearts were perfused for 240 min, and coronary angiography was performed after 120 min. The initial 120-min period was defined to replicate the average time observed in clinical practice between the beginning of NESP and the return to the transplant center where coronary angiography will be performed; the last two hours represented the duration needed for coronary angiography and preparation of the receiver in the operating room. Coronary angiography procedures were performed by two experienced interventional cardiologists. Mean aortic pressure and coronary flow were continuously monitored. Lactate levels were measured every 30 min to assess myocardial viability. Iomeprol volume and exposure to radiation were also recorded.
Baseline parameters are presented in Table 3. All hearts showed a favorable metabolic profile with preserved lactate extraction and were successfully preserved for 4 h on NESP. There were no premature endings due to perfusion failure. There was a failure in catheterizing the left coronary artery during the second procedure. In the third case, the views between the left and right coronary arteries were switched. The median volume of the contrast agent was 48 mL (min 38 mL-max 108 mL). The median dose of ionizing radiation was 3.30 mGy (min 1.0 mGy-max 17 mGy), with a median Dose-Area Product (DAP) of 0.55 Gy/cm2 (min 0.18 Gy/cm2-max 2.05 Gy/cm2). The median exposure time to ionizing radiation was 9.50 min (IQR: 6.75-12.75). The average procedure duration was 34.5 min (± 21). Lactate profiles, coronary flow, aortic pressure, and metabolic results are shown in Table 4 and Figure 3.
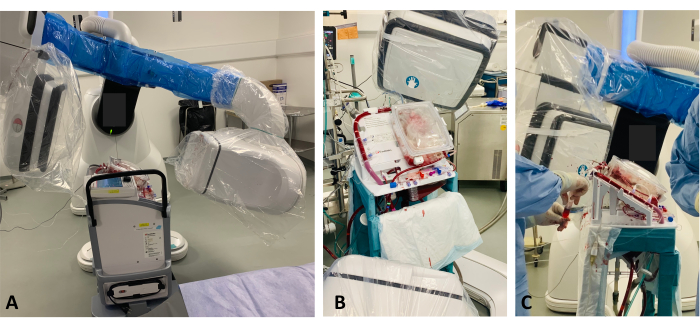
Figure 1: MP and fluoroscopic arm setup. (A) The MP is elevated by a platform so that the heart is within the X-ray field of the fluoroscopic arm to access the coronary angiography images. (B) After a 10 cm elevation, the MP is within the X-ray field, and coronary angiography images can be captured. (C) Operators performing coronary angiography through the valved orifice. Please click here to view a larger version of this figure.
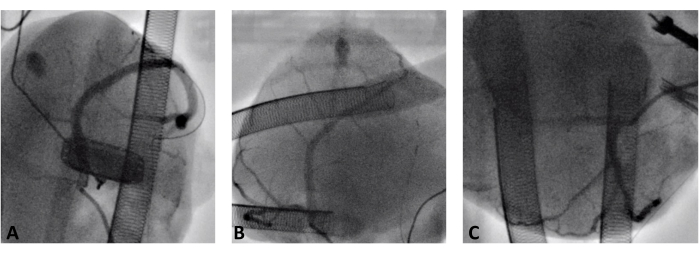
Figure 2: Coronary angiography during normothermic ex-situ heart perfusion. (A) Right coronary artery. (B) Left anterior descending artery. (C) Circumflex artery. Please click here to view a larger version of this figure.
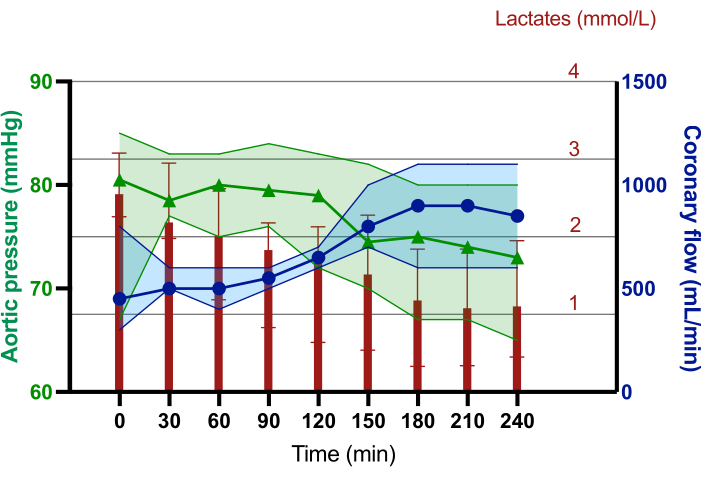
Figure 3: Median lactate levels, coronary flow, and aortic pressure trends during the 240 min of normothermic ex-situ heart perfusion. The red diagram bars represent the median lactate concentration in mmol/L. The blue line with dots represents the median coronary flow in mL/min. The green line with triangles represents the median aortic pressure in mmHg. The error bars represent 95% CI. Please click here to view a larger version of this figure.
| Solution | Components |
| Cardioplegia | 500 mL of Ringer solution |
| 10 mL of 10% KCl | |
| 3 mL of 2% Xylocaïne | |
| 6 mL of 20% Mannitol | |
| 6 mL of 8.4% Sodium Bicarbonate | |
| 7 mL of 15% Magnesium Sulfate | |
| Priming | 500 mL NaCl solution |
| 150 mg of Magnesium | |
| 250 mg of Methylprednisolone | |
| 1 g of Cefotaxime | |
| 50 UI of Insuline | |
| 5 mL of 30% Glucose | |
| Epinephrine infusion | 500 mL of 5% Glucose |
| 0.25 mg of epinephrine | |
| Adenosine infusion | 60 mg of Adenosine |
| 40 mL of NaCl solution |
Table 1: A detailed composition of the cardioplegia solution, priming solution, epinephrine, and adenosine infusions.
| Coronary arteries | Lateral rotation | Supero-inferior rotation |
| RCA | RAO 35 | CAU 44 |
| Proximal RCA | RAO 64 | CAU 38 |
| Distal RCA | RAO 65 | CAU 66 |
| Spider | RAO 70 | CAU 52 |
| LAD | RAO 135 | CAU 62 |
| LAD | RAO 167 | CAU 79 |
| Marginal artery | RAO 44 | CAU 51 |
| Cx | LAO 125 | CAU 83 |
Table 2: Coronary angiography views. RCA: Right Coronary Artery; LAD: Left Anterior Descending coronary artery; Cx: Circumflex artery; RAO: Right Anterior Oblique view; LAO: Left Anterior Oblique view; CAU: Caudal view.
| T0 | |
| Weight | |
| Pigs (kg) † | 51.9 (50.1—53.9) |
| Hearts (g) ‡ | 228.5 (± 30.1) |
| Timing (min) ‡ | |
| Heart retrieval | 13.5 (± 5.4) |
| Cold ischemic time | 41.8 (± 9.8) |
| Back-table time | 29.3 (± 8.2) |
| Perfusion parameters † | |
| Aortic Pressure (mmHg) | 80.50 (75.25—83.50) |
| Coronary flow (L/min) | 0.450 (0.375– 0.650) |
| Biological results † | |
| Lactates (mmol/L) | 2.59 (2.87—2.32) |
| pH ‡ | 7.44 (± 0.05) |
| pO2 (mmHg) | 523 (466–631) |
| pCO2 (mmHg) | 30.1 (26.2–35.8) |
| HCO3– (mmol/L) | 22.10 (17.55–24.37) |
| Natremia (mmol/L) | 143 (138.7–145.0) |
| Kaliemia (mmol/L) ‡ | 2.97 (± 0.60) |
| Calcemia (mmol/L) | 1.11 (1.09–1.16) |
| Glycemia (mmol/L) | 1.17 (1.12–1.34) |
Table 3: Baseline characteristics. †Data are expressed as medians (with IQR interquartile range).
‡Data are expressed as means (with standard derivations). T0 = at the beginning of the normothermic ex-situ heart perfusion; pO2 = oxygen partial pressure; pCO2 = carbon dioxide partial pressure; HCO3– = Bicarbonates.
| T120 | T240 | |
| Perfusion parameters | ||
| Aortic Pressure (mmHg) | 79.00 (74.2 – 82.2) | 73.00 (69.50 – 76.25) |
| Coronary flow (L/min) | 0.65 (0.60 – 0.70) | 0.85 (0.67 – 1.10) |
| Biological results | ||
| Lactates (mmol/L) | 1.68 (0.92 – 2.08) | 1.10 (0.61 – 1.75) |
| pH | 7.39 (7.35 – 7.42) | 7.36 (7.32 – 7.43) |
| HCO3- (mmol/L) | 22.10 (20.10 – 23.12) | 21.20 (19.22 – 22.92) |
| Natremia (mmol/L) | 144.5 (144.00 – 146.25) | 142.5 (137.50 – 145.25) |
| Kaliemia (mmol/L) | 3.55 (3.12 – 3.82) | 3.10 (2.97 – 3.62) |
| Calcemia (mmol/L) | 1.13 (1.11 – 1.16) | 1.10 (1.08 – 1.16) |
Table 4: Perfusion parameters and biological results before and 2 h after coronary angiography. Data are expressed as medians (with IQR interquartile range). T120 = 120 min after the beginning of the normothermic ex-situ heart perfusion, just before coronary angiography; T240 = 240 min after the beginning of the normothermic ex-situ heart perfusion, 120 min after coronary angiography; HCO3– = Bicarbonates.
