Source : Laboratoires de Jonas T. Kaplan et Sarah I. Gimbel — University of Southern California
Techniques d’imagerie cérébrale traditionnelle, à l’aide de MRI sont très bons à visualiser les structures bruts du cerveau. Une image de cerveau structurelle faite par l’IRM fournit un contraste élevé des frontières entre la matière grise et blanche et d’informations sur la taille et la forme des structures cérébrales. Cependant, ces images ne pas en détail la structure sous-jacente et l’intégrité des réseaux de matière blanche dans le cerveau, qui sont constitués de faisceaux d’axone qui interconnectent les régions cérébrales locales et éloignées.
Diffusion MRI utilise des séquences d’impulsions qui sont sensibles à la diffusion des molécules d’eau. En mesurant la direction de diffusion, il est possible de tirer des conclusions sur la structure des réseaux de la substance blanche du cerveau. Les molécules d’eau dans un axone sont limités dans leurs mouvements par la membrane cellulaire ; au lieu de passer au hasard dans toutes les directions avec une égale probabilité (mouvement isotrope), ils sont plus susceptibles de se déplacer dans certaines directions, en parallèle avec l’axone (mouvement anisotrope ; La figure 1). Par conséquent, des mesures de l’anisotropie de la diffusion sont censés reflètent les propriétés de la substance blanche tels que la densité de la fibre, l’épaisseur de l’axone et degré de myélinisation. Une mesure courante est fractionnaire anisotropie (FA). FA valeurs vont de 0, qui représente le mouvement complètement isotrope, à 1, ce qui reflète l’anisotropie maximale.
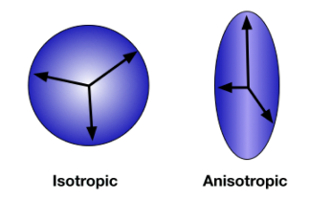
Figure 1 : Diffusion anisotropie. La direction de diffusion étant sans contrainte et aléatoire, mouvement est mesurée également dans toutes les directions. C’est isotrope diffusion (A). Lorsque les molécules d’eau sont contenus dans l’axone d’un neurone, la diffusion est anisotrope, tend à se produire plus fréquemment le long de la direction de l’axone (B). S’il vous plaît cliquez ici pour visionner une version agrandie de cette figure.
Dans cette expérience, nous utiliserons tenseur de diffusion (DTI) d’imagerie pour mesurer l’intégrité de la substance blanche dans le traumatisme crânien (TCC). TBI se produit lorsqu’une force extérieure blesse le cerveau comme un coup porté à la tête ou un mouvement brusque comme le genre qui peut-être se produire dans un accident de voiture. Ce type de lésion cérébrale de forces mécaniques est associé aux blessures-lésions axonales diffuses de la substance blanche dans le cerveau. Parce que c’est une blessure qui affectent l’intégrité de la substance blanche, les techniques de neuroimagerie standard peuvent ne pas révéler les dégâts. Toutefois, les mesures de diffusion sont particulièrement sensibles à ces changements anatomiques. Suite à une étude par Kraus et al. 1, on compare un groupe de contrôles sains à un groupe de personnes avec TBI et utilisation diffusion d’imagerie afin de mesurer l’effet des TCC sur la substance blanche cérébrale. En outre, nous allons tester la relation entre l’intégrité de la substance blanche et la fonction cognitive utilisant une tâche de l’attention. 2 cette étude utilise une zone d’approche d’intérêt (ROI) en se concentrant sur trois parcelles de matière blanche : le splenium du corps calleux, l’antérieure corona radiata et le faisceau longitudinal supérieur (Figure 2).
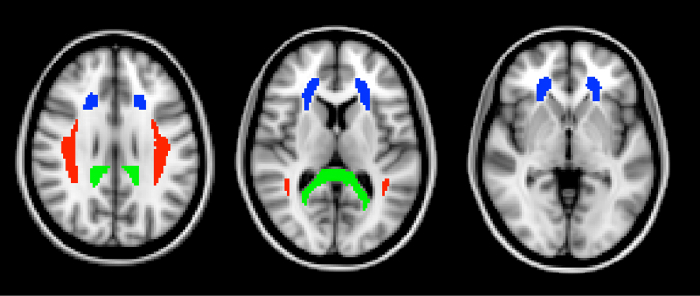
Figure 2 : régions d’intérêt. La trois ROIs, définie dans l’atlas ICBM DTI-81, apparaissent ici en tranches horizontales à travers le cerveau. En vert est le splenium du corps calleux. Le splenium est la partie la plus postérieure du corps calleux. En bleu est l’antérieur corona radiata. Le faisceau longitudinal supérieur est indiqué en rouge. S’il vous plaît cliquez ici pour visionner une version agrandie de cette figure.
The FA values from the three ROIs are shown in Figure 3. Fractional anisotropy was significantly lower in the TBI group in all three ROIs, indicating the presence of widespread white matter damage in those individuals. This non-localized loss of white matter integrity is typical of TBI.
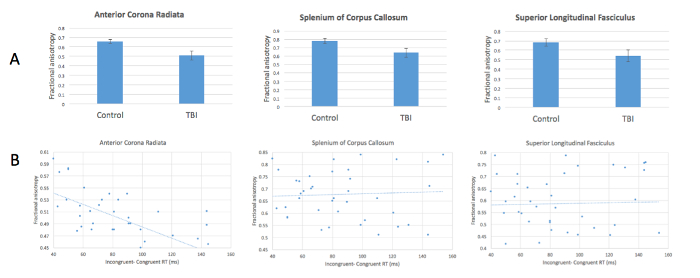
Figure 3: Reduced anisotropy in patients with TBI and relationship with attentional control. (A) FA values are significantly lower in TBI patients compared with healthy controls in all 3 ROIs. (B) FA in the anterior corona radiata correlates negatively with increased incongruency effect in the attention task. Please click here to view a larger version of this figure.
Our measure of attentional control-response time differences between congruent and incongruent targets-correlated negatively with FA values in the anterior corona radiata (Figure 3). In other words, greater differences in response time, indicating poorer attentional control, are associated with decreased FA. These results evidence a relationship between white matter integrity in this location and performance on this task. This relationship was not found in the other two ROIs. The anterior corona radiata is associated with connections to the anterior cingulate cortex, a structure known to play an important part in attentional control.