Fonte: Laboratori di Jonas T. Kaplan e Sarah I. Gimbel—University of Southern California
Le tradizionali tecniche di imaging cerebrale che utilizzano la risonanza magnetica sono molto brave a visualizzare le strutture grossolane del cervello. Un’immagine cerebrale strutturale realizzata con la risonanza magnetica fornisce un elevato contrasto dei confini tra materia grigia e bianca e informazioni sulle dimensioni e la forma delle strutture cerebrali. Tuttavia, queste immagini non descrivono in dettaglio la struttura sottostante e l’integrità delle reti di materia bianca nel cervello, che consistono in fasci di assoni che interconnettono regioni cerebrali locali e distanti.
La risonanza magnetica a diffusione utilizza sequenze di impulsi sensibili alla diffusione di molecole d’acqua. Misurando la direzione di diffusione, è possibile fare inferenze sulla struttura delle reti di materia bianca nel cervello. Le molecole d’acqua all’interno di un assone sono vincolate nei loro movimenti dalla membrana cellulare; invece di muoversi casualmente in ogni direzione con uguale probabilità (movimento isotropo), è più probabile che si muovano in determinate direzioni, in parallelo con l’assone (movimento anisotropico; Figura 1). Pertanto, si ritiene che le misure di anisotropia di diffusione riflettano le proprietà della sostanza bianca come la densità delle fibre, lo spessore degli assoni e il grado di mielinizzazione. Una misura comune è l’anisotropia frazionaria (FA). I valori di FA vanno da 0, che rappresenta il movimento completamente isotropo, a 1, riflettendo l’anisotropia massima.
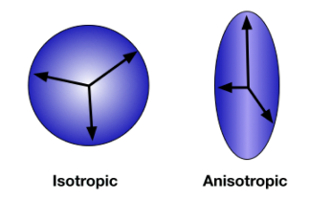
Figura 1: Anisotropia di diffusione. Quando la direzione di diffusione è libera e casuale, il movimento viene misurato in tutte le direzioni allo stesso modo. Questa è la diffusione isotropa (A). Quando le molecole d’acqua sono contenute all’interno dell’assone di un neurone, la diffusione è anisotropa, tendendo a verificarsi più frequentemente lungo la direzione dell’assone (B). Fare clic qui per visualizzare una versione più grande di questa figura.
In questo esperimento useremo l’imaging del tensore di diffusione (DTI) per misurare l’integrità della sostanza bianca nella lesione cerebrale traumatica (TBI). Il TBI si verifica quando una forza esterna ferisce il cervello, come un colpo alla testa o un movimento improvviso come quello che potrebbe verificarsi in un incidente d’auto. Questo tipo di lesione cerebrale da forze meccaniche è associato a lesioni assonali diffuse-danno alla sostanza bianca in tutto il cervello. Poiché si tratta di una lesione che colpisce l’integrità della sostanza bianca, le tecniche di neuroimaging standard potrebbero non rivelare il danno. Tuttavia, le misure di diffusione sono particolarmente sensibili a questi cambiamenti anatomici. A seguito di uno studio di Kraus et al. 1, confrontiamo un gruppo di controlli sani con un gruppo di persone con TBI e utilizziamo l’imaging a diffusione per misurare l’effetto del TBI sulla sostanza bianca cerebrale. Inoltre, testeremo la relazione tra integrità della sostanza bianca e funzione cognitiva utilizzando un compito di attenzione. 2 Questo studio utilizza un approccio di regione di interesse (ROI) incentrato su tre tratti di sostanza bianca: lo splenio del corpo calloso, la corona radiata anteriore e il fascicolo longitudinale superiore (Figura 2).
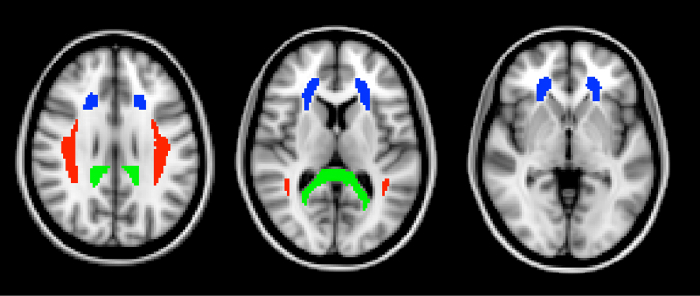
Figura 2: Regioni di interesse. I tre ROI, definiti dall’atlante ICBM DTI-81, sono mostrati qui in sezioni orizzontali attraverso il cervello. In verde è lo splenio del corpo calloso. Lo splenio è la parte più posteriore del corpo calloso. In blu è la corona radiata anteriore. Il fascicolo longitudinale superiore è mostrato in rosso. Fare clic qui per visualizzare una versione più grande di questa figura.
The FA values from the three ROIs are shown in Figure 3. Fractional anisotropy was significantly lower in the TBI group in all three ROIs, indicating the presence of widespread white matter damage in those individuals. This non-localized loss of white matter integrity is typical of TBI.
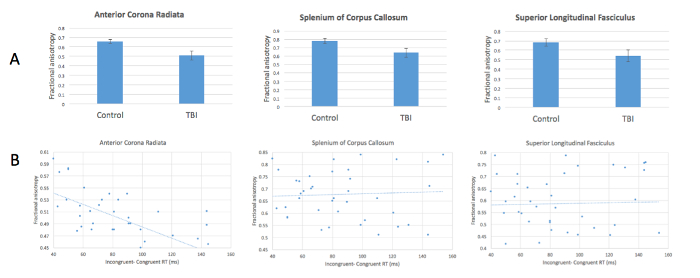
Figure 3: Reduced anisotropy in patients with TBI and relationship with attentional control. (A) FA values are significantly lower in TBI patients compared with healthy controls in all 3 ROIs. (B) FA in the anterior corona radiata correlates negatively with increased incongruency effect in the attention task. Please click here to view a larger version of this figure.
Our measure of attentional control-response time differences between congruent and incongruent targets-correlated negatively with FA values in the anterior corona radiata (Figure 3). In other words, greater differences in response time, indicating poorer attentional control, are associated with decreased FA. These results evidence a relationship between white matter integrity in this location and performance on this task. This relationship was not found in the other two ROIs. The anterior corona radiata is associated with connections to the anterior cingulate cortex, a structure known to play an important part in attentional control.