This protocol is reproducible and mimics OAGB as practiced on humans. The safety of this protocol is supported with published data23,24 with a low mortality rate between 12% and 25%. Different surgeons in the research team with a similar mortality rate have practiced this protocol.
Nonetheless, learning rodent surgery is complex, and the use of magnifying glasses is mandatory. Indeed, the critical step of the construction of a microscopic anastomosis requires a learning period from around 15 to 20 operations to reach an optimal dexterity. A surgical defect can lead to an anastomotic leakage of a gastric obstruction, which is the main death cause in our experience. Another key to success is the postoperative nutrition; indeed, an early postoperative solid nutrition can be dangerous. This protocol also provides a precise postoperative nutrition protocol, which has been demonstrated to be safe. The concept of this surgery on humans and on rats is illustrated in Figure 1. A result of the operation after sacrifice is provided in Figure 2.
Results obtained on weight loss after operation on obese rats were quite similar to those observed in humans, with a body weight loss of about 20%, stable after the operation. The results are detailed in Figure 3. Better insulin sensitivity and glucose tolerance were observed as soon as 2 weeks after the surgery, as assayed by an oral glucose test (OGTT) and an insulin tolerance test (ITT). These results are detailed in Figure 4. HFD-induced obesity has been described to promote insulin resistance and glucose intolerance in Wistar rats25; comparable data have been gathered in our unit (unpublished). Wistar rats are not a model of type 2 diabetes.
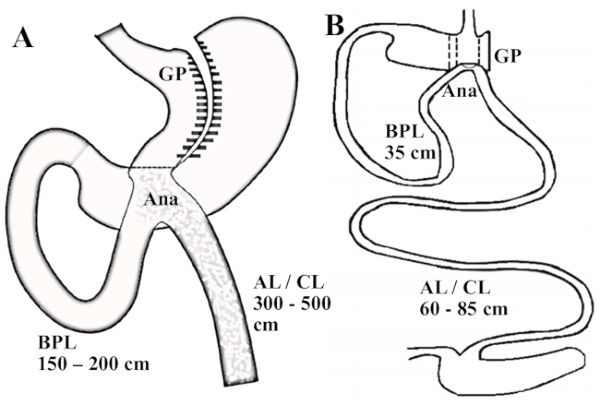
Figure 1: Illustration of OAGB on humans and on this rat model. (A) Scheme of an OAGB in humans; the gastric pouch is long and tubular and the BPL measures between 150 and 200 cm. (B) Rat model of an OAGB. The ratio of the BPL and the AL/CL reproduce the one practiced for human surgery; the BPL measures 35 cm. Abbreviations: GP = gastric pouch; Ana = anastomosis; AL = alimentary limb; CL = common limb. Please click here to view a larger version of this figure.
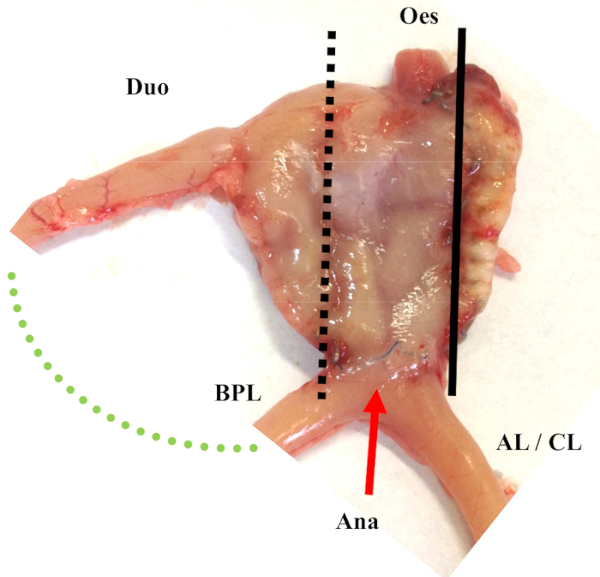
Figure 2: Illustration of OAGB on rats after sacrifice. Abbreviations: GP = gastric pouch; Ana = anastomosis; AL = alimentary limb; CL = common limb; Oes = Esophagus; Duo = duodenum Please click here to view a larger version of this figure.
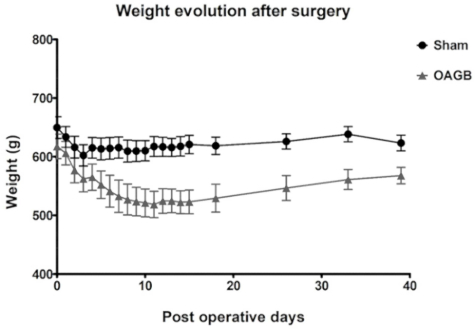
Figure 3: Postoperative weight evolution (median ± SD) after OAGB and sham surgery. The sham surgery consisted of a laparotomy and a pinch on the great gastric curve with non-traumatic forceps. Please click here to view a larger version of this figure.
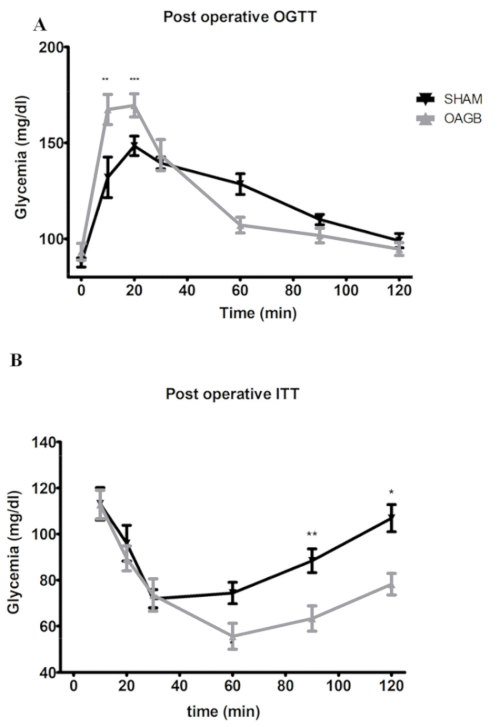
Figure 4: Glucose metabolism after OAGB and sham surgery; post-operative OGTT and ITT. (A) Post-operative OGTT. OAGB and sham rats were made to fast before being subjected to an oral glucose tolerance test (OGTT: 1 g/kg of body weight). (B) Post-operative ITT: an injection of 1 U insulin/kg of body weight. Rats were made to fast 4 h before receiving the insulin injection. Blood was harvested in the tail vein at t = 0 and at 10, 20, 30, 60, and 120 min after the insulin or glucose administration. Glucose was measured using a blood glucose meter. Glycemia was expressed in mg/dL ± standard deviation. Abbreviations:OGTT = oral glucose tolerance test; ITT = insulin tolerance test; BW = body weight. * p < 0.05, ** p < 0.01, *** p < 0.001; after two-way ANOVA statistical test. The sham surgery consisted of a laparotomy with a nontraumatic pinch of the great gastric curve using non-traumatic forceps. All data are presented as mean ± SD. Please click here to view a larger version of this figure.