We looked at the contribution of the single liver lobes to the total liver volume and found that the LLL represents 33% of the total liver volume. The ML represents 32% of the total liver volume, the RSL 13%, the RIL 10%, and the CL 10% (Table 2). The boxplots show that the relative contribution of the liver lobes is comparable between the different mice of the same strain (Figure 3B). Hence, a resection of the LLL results in a resection of 35% of the total liver volume, and a resection of the LLL and ML results in a resection of 66% of the total liver volume. As resection of the independent liver lobes to measure weight for contribution to total liver volume occurred postmortem, the value measured is most likely a slight overrepresentation of actual resection weight that can be achieved when performing surgery on a living mouse. This is because the ligature is placed slightly decentral (especially when performing a resection of the ML) to prevent obstruction of the vena cava.
Further experiments show that resection has an impact on the weight of the reference lobe, which is the RIL. The mean weight of the RIL was 0.49% of the total body weight in those mice that did not receive a resection. After performing a resection of the LLL (= Minor Resection), the mean weight increased to 0.82% of the total body weight; this difference was significant (p < 0.0001). After performing a resection of the LLL and ML (= Major Resection), the weight of the RIL increased to a mean of 0.99% of the total body weight. The difference between no resection and a large resection (LLL + ML resection) was also significant (p < 0.0001). However, the difference between the resection of the LLL and the combined LLL + ML resection was not significant (Figure 3C).
In a further experiment, we looked at the increase in the weight of the different liver lobules in addition to the increase of the RIL weight after a minor or major resection. This is of pronounced interest as we chose to inject the tumor organoids into the RSL. After performing a major resection, we saw a pronounced increase in the weight of the RSL in relation to the body weight of the mouse compared to the RIL (Figure 3D,E). The mean weight of the RSL was 1.73% of the mouse body weight, which was significantly larger than the mean weight of 0.99% of the mouse body weight for the RIL (p = 0.0053).
Finally, we report the histology and immunohistochemical staining of two separate HCC tumors and the subsequent patient-derived organoid (PDO) line and resulting mouse tumor. The first case depicted in Figure 4A shows a poorly differentiated HCC with neuroendocrine differentiation. The tumor stage after operation was pT2 pN0 (0/15) L0 V1 Pn1 R0. The patient had recurrent disease 3 months after the operation in the remaining liver tissue and distant metastasis in the lung. H/E and immunohistochemistry staining (Figure 4A) typical for HCC showed that the PDO resembles the morphological features of the original patient tumor. The same is also true for the mouse tumor: it resembles the PDO and the original patient tumor. The second case depicted in Figure 4B shows a poorly differentiated HCC (Grade 3 Edmondson). The original Tumor grade after resection was pT4 pN0 (0/5) L1 V1 Pn0 G3 R0. Again, the staining shows that the PDO resembles the original patient's tumor, and the mouse tumor resembles the patient's tumor and the PDO (Figure 4B). Figure 5A-E show PDO development from passages 1 to 18.

Figure 1: Flowchart of the experimental setup. In the first step, the organoids will be injected into the right superior lobe via laparotomy. Until the second step, monitoring of the tumor growth is done with sonography at an interval of 2 weeks. In the second step, mice will be randomized into three groups: control (no resection), 30% resection, and 65% resection. After resection, the tumor is sonographically monitored until it reaches the termination criteria. Please click here to view a larger version of this figure.

Figure 2: Liver lobules and positioning of retractors and ligature for lobe resection. (A) Positioning of retractors that improves the exposure of the cranial abdomen where the liver lobules are located (ventral-dorsal view). (B) Positioning of retractors (caudaln-cranial view). (C) Schematic of liver lobules located in the cranial abdomen as seen during surgery; the ligament between the LLL and the caudate lobe is exposed when the LLL is flipped cranially. It is important to dissect this ligament to prohibit bleeding through tearing forces when left in place and to ensure good central positioning of ligature for removal of the LLL. (D) Positioning of ligature for resection of the LLL (it is important to close the ligature by pulling the caudal free end of the ligature and not both free ends equally in opposite directions. If both ends are pulled equally, there is a risk of perforating the diaphragm with the cranial forceps. It also helps to use blunt forceps to hold the cranial free end in position. Abbreviations: LML = Left Middle Lobe; RML = right middle lobe; RIL = Right Inferior Lobe; RSL = Right Superior Lobe; LLL = Left Lateral Lobe; CL = caudate lobe; Lig = ligament. Please click here to view a larger version of this figure.

Figure 3: Percentage of total liver volume contributed by liver lobules and lobe regeneration after resection. (A) Schematic of liver lobules showing the percentage of total liver volume contributed by each liver lobule. (B) Bar plots showing the contribution of liver lobules to total liver volume, (C) Results showing the increase in weight of the reference lobe (Right Inferior Lobe) after 30% and 65% resection. (D) Regeneration in the RSL after major resection (the regeneration in the RSL is more pronounced compared to the right inferior lobe. Results demonstrate the difference in weight increase between Right superior and Right inferior after 65% resection). (E) Demonstration of size difference between Right superior and Right inferior lobules. Top row corresponds to the Right superior lobe and the bottom row corresponds to the Right inferior lobe. Abbreviations: ML = Middle Lobe; RSL = Right Superior Lobe; RIL = Right Inferior Lobe; LLL = Left Lateral Lobe; AC = Anterior caudate lobe; PC = and Posterior Caudate Lobes; IVC = Inferior Vena Cava. Please click here to view a larger version of this figure.
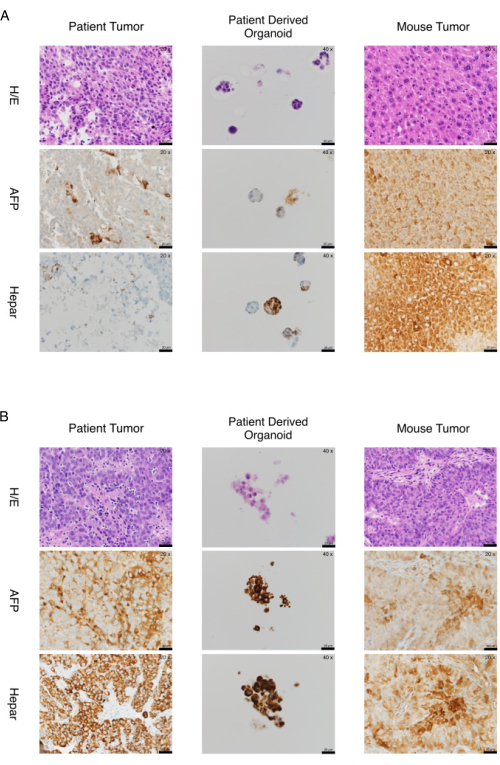
Figure 4: Two cases of marker expression in organoids and tumors from patient-derived xenografts. (A) Expression of markers in organoids and tumors from patient-derived xenograft-a case. The organoids and tumors from the xenograft recapitulate the expression of immunohistochemistry markers of the original tissue. Histology and immunohistochemical staining AFP and Hepar of Case p151-poorly differentiated HCC (Edmondson Grade III) with neuroendocrine differentiation. Microphotographs of patient tumor (20x), organoids (40x), and tumor (20x) obtained from the mouse model are shown in the left, middle, and right columns, respectively. Hematoxylin/Eosin staining and immunohistochemical staining for AFP and Hepar are shown in the top, middle, and bottom rows, respectively. (B) Expression of markers in organoids and tumors from patient-derived xenograft-a second case. The organoids and tumors from the xenograft recapitulate the expression of immunohistochemistry markers of the original tissue. Histology and immunohistochemical staining AFP and Hepar of Case p220-poorly differentiated HCC (Edmondson Grade III). Microphotographs of patient tumor (20x), organoids (40x), and tumor (20x) obtained from the mouse model are shown in the left, middle, and right columns, respectively. Hematoxylin/Eosin staining and immunohistochemical staining for AFP and Hepar are shown in the top, middle, and bottom rows, respectively. Scale bars = 20 µm. Abbreviations: H/E = hematoxylin/eosin; HCC = hepatocellular carcinoma; AFP = alpha fetoprotein. Please click here to view a larger version of this figure.
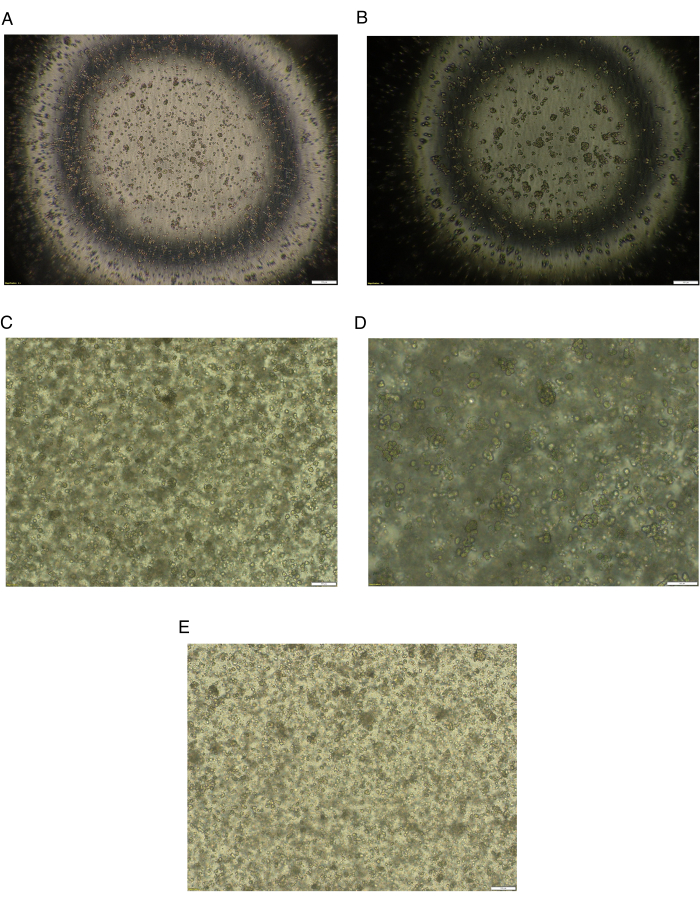
Figure 5: Brightfield images of HCC cells through several passages. (A) Brightfield image of HCC cells after patient's HCC tissue digestion and after plating at day 0. Magnification 4x, scale bar = 200 µm. (B) Brightfield image of HCC cells 48 h after the first plating. Formation of small organoids. Magnification 4x, scale bar = 200 µm. (C) Brightfield image of HCC organoids at passage 15. Magnification 4x, scale bar = 200 µm. (D) Brightfield image of HCC organoids at passage 15. Magnification 10x, scale bar = 100 µm. (E) Brightfield image of HCC organoids at passage 18 after defrosting. Magnification 4x, scale bar 200 µm. Abbreviation: HCC = hepatocellular carcinoma. Please click here to view a larger version of this figure.
| Dissociation Buffer | Add to 5 mL of Ad-DF+++ : | |||
| o 236 µL of Collagenase IV (50 mg /mL or 11653 U/mL); 202.6 mg of Collagenase IV in 4 mL of 0.15 M NaCl. Filter with 0.22 µm filter and stored at -20 °C. | ||||
| o 10 µL of DNAse (10,000 Kunitz U/mL); 11 mg (2,824 U/mg) in 3 mL of 0.15 M NaCl. Filter with 0.22 µm filter and stored at -20 °C. | ||||
| o 14 µL of Hyaluronidase (339 kU/mL); 191.3 mg in 2 mL of 0.15 M NaCl. Filter with 0.22 µm filter and stored at -20 °C. | ||||
| o 333 µL of BSA; 1 g in 100 mL of 0.15 M NaCl (1% Stock Solution). Filter with 0.22 filter and stored at -20 °C. | ||||
| o 1 µL of 10 mM stock of ROCK Inhibitor | ||||
| Cell suspension freezing medium | To 35 mL of RPMI medium, add 10 mL of FBS and 5 mL of DMSO | |||
| Mix well and aliquot 5 mL in 15 mL tube | ||||
| Store at -20 °C | ||||
| Ad-DF+++ | To 500 mL of adDMEM/F12, add | |||
| o 5 mL of GlutaMAX | ||||
| o 5 mL of HEPES 1 M | ||||
| o 5 mL of Pen-Strep | ||||
| Can be stored at 4 °C for 4 weeks | ||||
Table 1: Solutions for tissue dissociation and organoid generation.
| Mouse Number | Left Lateral | Medial | Superior Right | Inferior Right | Anterior + Posterior Caudate |
| Mouse 1 | 32.317 | 30.894 | 13.618 | 13.211 | 9.959 |
| Mouse 2 | 38.697 | 30.143 | 12.220 | 10.387 | 8.554 |
| Mouse 3 | 32.665 | 32.265 | 12.625 | 11.824 | 10.621 |
| Mouse 4 | 30.000 | 36.721 | 12.623 | 9.508 | 11.148 |
| Mouse 5 | 31.562 | 34.944 | 13.849 | 10.145 | 9.501 |
| Mouse 6 | 32.203 | 35.593 | 14.068 | 9.661 | 8.475 |
| Mouse 7 | 35.591 | 28.504 | 13.071 | 11.496 | 11.339 |
| Mouse 8 | 34.773 | 32.045 | 13.864 | 8.636 | 10.682 |
| Mouse 9 | 33.167 | 41.128 | 7.960 | 7.794 | 9.950 |
| Mouse 10 | 31.751 | 31.751 | 16.367 | 9.493 | 10.638 |
| Median | 32.491 | 32.155 | 13.344 | 9.903 | 10.290 |
| IQR | 2.908 | 4.485 | 1.225 | 2.000 | 1.069 |
Table 2: Results of an experiment showing weight distribution of the different mouse liver lobules. The results demonstrate that the left lateral lobe and middle lobe are consistently the biggest lobules combining to an average of 65% of the total liver volume. Abbreviation: IQR = interquartile range.
