From January 2021 to June 2022, we selected 114 patients who underwent radiofrequency ablation of atrial fibrillation at our hospital. Patients were excluded based on the following criteria: no 3D volume reconstruction image of left atrial CT (n = 11), no transseptal puncture ICE image (n = 4), and incomplete reconstruction of the left atrium and pulmonary vein images (n = 4). Finally, 50 patients with ICE 3D modeling and 45 with FAM 3D modeling as control group was included in this study.
Two professional electrophysiologists analyzed all the 3-D modeling images. We compared the degree of anatomical anastomosis between Carto modeling and left atrial computed tomography angiography imaging. The 3D images of FAM modeling and refined ultrasound modeling (Figure 1) were scored (0 points: completely inconsistent; 5 points: completely consistent). The transseptal puncture position appropriateness (Figure 2) was scored for conventional and refined ultrasound-guided methods (0 points: totally inappropriate, requiring re-puncture; 5 points: Very appropriate). The maximum cross-sectional area of the pulmonary vein vestibule gathered using conventional and refined ultrasound modeling was compared with the maximum cross-sectional area obtained by left atrial CT. The modeling observer scores were 3.40 ± 0.81 and 3.02 ± 0.72 (P < 0.05) in the ICE and FAM groups, respectively. The observer scores for selecting transseptal puncture sites were 4.62 ± 0.73 and 4.29 ± 0.97 (P < 0.05) in the ICE and FAM groups, respectively (Figure 3). The pulmonary vein antrum area acquired using the ICE- and FAM-based methods correlates with the area acquired by left atrial CT. However, the 95% confidence interval bias was narrower in ICE-acquired models than in FAM-acquired models using Bland-Altman analysis (-238 cm2 to 323 cm2 Vs. -363 cm2 to 386 cm2, respectively)(Figure 4).
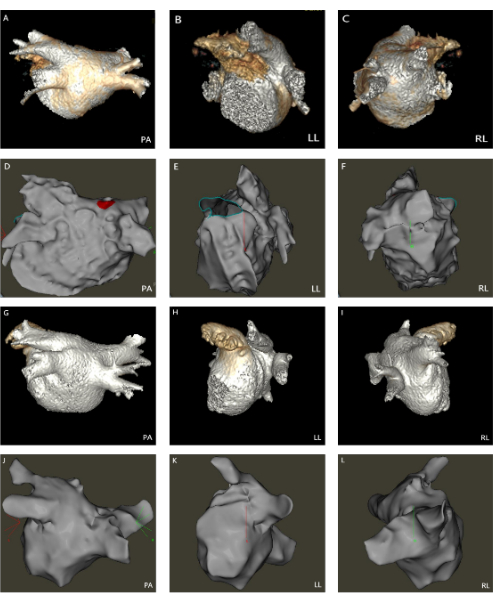
Figure 1: 3D modeling images of the left atrium, pulmonary vein, and transseptal puncture. (A–F) Comparison of the 3D modeling of ICE and left atrial CT. (G–L) Comparison of the 3D modeling of FAM and left atrial CT. (PA: Posterior-anterior; LL: Left lateral; RL: Right lateral). Please click here to view a larger version of this figure.
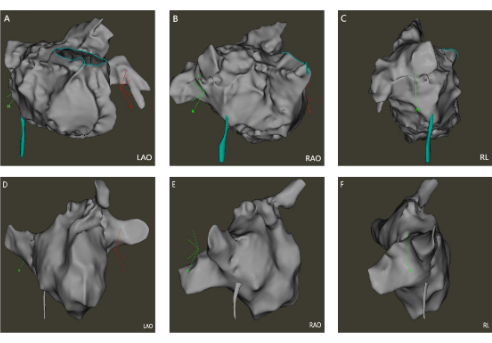
Figure 2: The transseptal puncture positioning maps. (A–C) The ICE-guided transseptal puncture positioning maps; (D–F) The FAM-guided transseptal puncture positioning maps. (LAO: Left anterior oblique; RAO: Right anterior oblique; RL: Right lateral). Please click here to view a larger version of this figure.
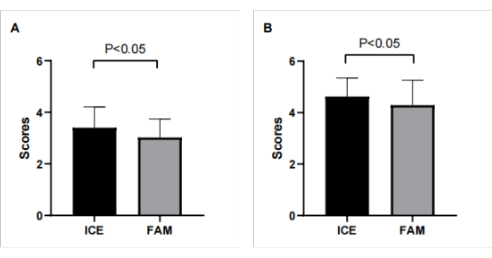
Figure 3: The observer scores for modeling and selecting transseptal puncture sites. (A) The observer scores for modeling in the ICE and FAM groups were 3.40 ± 0.81 and 3.02 ± 0.72 (P < 0.05), respectively; (B) The observer scores for selecting transseptal puncture sites in the ICE and FAM groups were 4.62 ± 0.73 and 4.29 ± 0.97 ( P < 0.05), respectively. Please click here to view a larger version of this figure.
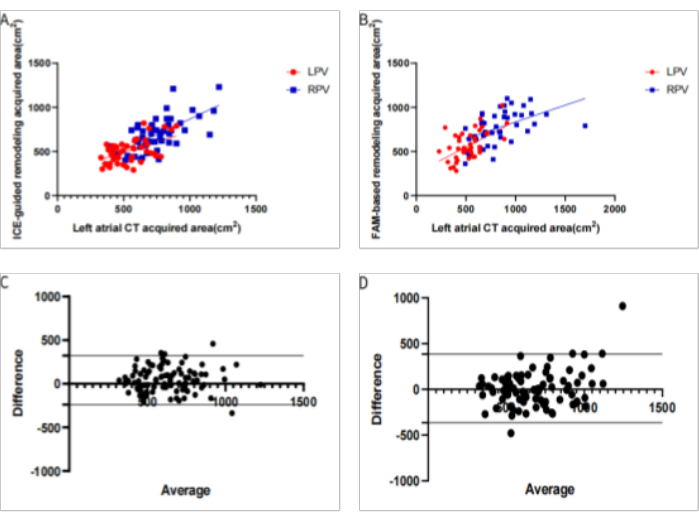
Figure 4: Comparison of the two modeling methods for measuring the pulmonary vein area. (A) Linear regression analysis of the pulmonary vein antrum area acquired using the ICE-based method and left atrial CT; (B) Linear regression analysis of the pulmonary vein antrum area obtained by the FAM-based method and left atrial CT; (C) Bland-Altman plots of the ICE-acquired models compared to the left atrial CT. The 95% confidence interval bias was -238 cm2 to 323 cm2; (D) Bland-Altman plots of the FAM-acquired models compared to the left atrial CT. The 95% confidence interval bias was -363 cm2 to 386 cm2. (LPV: Left pulmonary vein; RPV: Right pulmonary vein Please click here to view a larger version of this figure.
Video 1: Specific process for marking important anatomical locations. Please click here to download this File.
