1. Preparation of PBMC
- Procedures for good aseptic technique and universal precautions must be adhered to during the conduct of this protocol.
- Isolate PBMC from healthy volunteer donors by density gradient centrifugation using Ficoll-Hypaque. Alternatively cryopreserved PBMC can be resuscitated.
- Count viable PBMC after staining with Trypan Blue using a hemocytometer. Resuspend PBMC in complete culture media (CM) at a concentration of 1 million viable cells/mL in a 15mL Falcon tube.
2. Setting Up the Bulk Alloanergizing Co-culture
- PBMCs from two separate donors are needed to set up the alloanergization cultures. Cells from one donor will serve as the responder and cells from another donor will serve as the stimulator (termed the First Party stimulator).
- Place 10 million stimulator PBMC at 1 million/ml in a 15 mL Falcon tube and add 100mg of anti-B7.1 and 100mg of anti B7.2 antibodies to block costimulation. Gently agitate the tube and incubate for 30 minutes. Incubation conditions for this and all subsequent steps are 37°C/5% CO2/80% humidity
- Irradiate stimulator PBMC (33 Gy) and add to a T-25 50cm3 cell culture flask with a gas-permeable cap. Label the flask “Bulk alloanergizing co-culture”.
- Add 10mL of responder PBMC (at 1 million/ml in CM) to the flask.
- Add a further 100mg each of anti-B7.1 and anti B7.2 antibodies and mix gently prior to placing the flask upright in an incubator for 72 hours
3. Setting Up the Bulk Control Co-culture
- Place 10 million stimulator PBMC (at 1 million/ml) in a 15mL Falcon tube.
- Irradiate 10 million stimulator PBMC (33 Gy).and add to a 50cm3 cell culture flask. Label “Bulk control co-culture”.
- Add 10mL of responder PBMC at 1 million/ml in CM to the flask and mix gently prior to placing the flask upright in an incubator for 72 hours.
4. Setting Up the Primary Mixed Lymphocyte Reaction (MLR) to Measure the Efficacy of Co-stimulatory Blockade
- The efficacy of costimulatory blockade is measured in a primary MLR which is set up using PBMC from the bulk alloanergizing and control co-cultures
- The primary MLR is set up on the same day that the bulk cultures have been set up
- First label one U bottomed 96 well plate “Primary MLR” for each of the three time points to be measured (Day 4, 5 and 6 after plates are set up).
- Decant 5mL from each of the bulk control and alloanergizing co-cultures into 15mL Falcon tubes.
- Pipette 200mL of cell suspension from each Falcon tube into triplicate wells on each plate. Label these wells “no costimulatory blockade (CSB)” for the cells from the bulk control co-cultures and “CSB” for the cells from the bulk alloanergizing co-cultures
- Add 200mL of CM to 6 wells on each plate as negative controls. 200mL PBS is added to all empty wells to reduce evaporation. Place plates in the incubator.
5. Setting Up the Secondary MLR to Measure the Efficacy of Alloanergization
- 72 hours after setting up the bulk co-cultures, residual alloresponses in alloanergized PBMCs are measured in a secondary MLR. In the secondary MLR, PBMC from both the bulk alloanergizing co-culture and the bulk control co-culture are washed and restimulated with irradiated allostimulator PBMC
- To set up the secondary MLR label one U bottomed 96 well plate “Secondary MLR” for each of the three time points to be measured (Day 3, 5 and 7 after set up).
- Remove 5mL from each of the bulk control and alloanergizing co-cultures, transfer to 15mL Falcon tubes and centrifuge for 5-10 minutes at 2000 rpm.Aspirate the supernatant carefully, disrupt the pellet, add 10mL of CM and centrifuge the cells again. Repeat this washing step.
- Resuspend the cells in 1mL of CM. Count the viable cells using Trypan Blue staining, and adjust the cell concentration to 1 million viable responder cells/mL.
- Pipette 100mL of cell suspension from each Falcon tube into triplicate wells of each plate. Label these wells “First Party (FP) allorestimulation”
- Pipette 100mL of cell suspension from each Falcon tube into a further 3 wells on each plate and label these wells “CD3/28 stimulation”
- To prepare stimulator cells for the secondary MLR, isolate PBMC from fresh blood (or resuscitate cryopreserved PBMC) from the same healthy donor used to supply first party stimulator PBMCs in the alloanergizing and control cultures.
- Suspend PBMC from the FP donor at a concentration of 1 million/mL and irradiate (33Gy)
- Add 100mL of irradiated stimulator cells to wells labeled “FP allorestimulation”
- For positive controls, add 1 mL each of CD3 and CD28 monoclonal antibodies and 98mL of CM to wells labeled “CD3/28 stimulation”. Add 200 mL of CM to 6 wells on each plate as a negative control and 200mL of PBS to empty wells. Place the plates in the incubator.
6. Measuring the Specificity of Alloanergization
- The specificity of alloanergization is determined by comparing proliferation of responder cells taken from the completed alloanergizing and control co-cultures after stimulation with irradiated PBMC obtained from a “third party” healthy donor (i.e. a different donor to the First Party) in a secondary MLR.
- Label three 96 well plates “Secondary MLR Specificity” Day 3, 5 and 7.
- Remove 5mL from each of the bulk control and alloanergizing co-cultures transfer to 15mL Falcon tubes and centrifuge for 5-10 minutes at 2000 rpm. Aspirate the supernatant carefully, disrupt the pellet, add 10mL of CM and centrifuge the cells again. Repeat this washing step.
- Resuspend the cells in 1mL of CM. count using Trypan Blue staining, and adjust the cell concentration to 1 million viable responder cells/mL.
- To prepare third party stimulator cells for the secondary MLR, isolate PBMC from fresh blood (or resuscitate cryopreserved PBMC) from a new healthy donor. Pipette 100mL of cell suspension from each Falcon tube into triplicate wells of each plate. Label these wells “TP allostimulation”
- Suspend PBMC from a TP donor at 1 million/mL and irradiate (33 Gy)
- Add 200mL of irradiated TP stimulator cells to wells labeled “TP allostimulation”
- The specificity of alloanergization may also be determined by comparing proliferation of responder cells taken from the completed alloanergizing and control co-cultures after stimulation with an infectious pathogen such as CMV. For this step it is essential to use responder PBMC from donors with previously demonstrated proliferative responses to CMV lysate.
- Label three 96 well plates “Secondary MLR CMV” Day 3, 5 and 7.
- To prepare the responder cells for the secondary MLR to measure CMV responses, transfer 5 ml from each of the bulk control and alloanergizing co-cultures to 15 ml tubes and wash, count and resuspend at 1 million cells/ml in CM as previously described.Pipette 100mL of cell suspension from each Falcon tube into a 3 wells on each plate.
- Add 0.1 mL of CMV lysate in 100ul CM to wells
- Add 200 mL of CM to 6 wells on all plate as a negative control and add 200mL of PBS to empty wells. Place the plates in the incubator.
7. Measuring Proliferation in the Primary and Secondary MLRs
- Responder cell proliferation is measured by thymidine incorporation assay in the primary and secondary MLRs. Proliferation is measured at Day 4, 5 and 6 after the Primary MLR plates are set up and at Day 3, 5 and 7 after the Secondary MLR plates are set up.
- 1mCi of tritiated thymidine is added to wells 16 hours prior to harvesting
- After the addition of tritiated thymidine, the plate is incubated for a further16 hours then harvested onto a filter mat using a Tomtec harvester (or similar). Air-dry the filtermat for one hour then place in a sample bag, add 5 mL scintillation fluid and seal. Read the plate in a Wallac Micro beta scintillation counter or similar.
8. Calculating the Efficacy of Co-stimulatory Blockade in the Primary MLR
- The percentage inhibition (PI) of primary alloresponses is calculated as 100 x [mean cpm in allostimulation wells (bulk alloanergy co-culture PBMC) – mean cpm in allostimulation wells (bulk control co-culture PBMC)}

9. Calculating the Efficacy of Alloanergization in the Secondary MLR
The PI of secondary alloresponses is calculated as

10. Calculating the Specificity of Alloanergization in the Secondary MLR
- After restimulation of cells with CD3 and CD28, TP allostimulators or CMV antigen, the PI of responses to these stimuli may also be calculated using this formula. This gives a measure of the specificity of the alloanergization process
11. Generating Alloanergized Donor PBMC for Clinical Use After Allogeneic Hematopoietic Stem Cell Transplantation (HSCT)
- Alloanergized donor PBMC may be generated for clinical use after HLA-mismatched allogeneic HSCT using the protocol outlined above
- When generating cells for clinical use, responder PBMC are obtained from the HSCT donor and stimulator PBMC from the HSCT recipient prior to transplant.
- When generating PBMC for clinical use, all steps are performed under Good Manufacturing Process conditions in accredited stem cell processing facilities.
- Additional quality control assays are performed including endotoxin assays and gram stain and culture to meet safety criteria prior to the release of cells for clinical use
12. Representative Results
Using HLA-mismatched stimulator and responder PBMC, the presence of costimulatory blockade in the primary MLR reduces mean alloproliferation of responder PBMC at Day 5 to around 30% (+/- 10%, mean +/- standard deviation) of that seen in control primary MLR in the absence of costimulatory blockade. This is equivalent to a mean inhibition of primary alloproliferation of around 70% (+/- 10%) at D5, Figure 1 A and B.
In the secondary MLR at Day 5, FP alloproliferation of alloanergized PBMC is typically 10-15% (+/- 10%) of that seen with control PBMC equivalent to a mean inhibition of proliferation of 85-90% (+/- 10%), Figure 2A and B. This demonstrates that alloanergized PBMC are hyporesponsive to FP allostimulators.
In contrast alloanergized PBMC typically retain 70-100% of their proliferation to mitogens (CD3/CD28 antibodies), TP allostimulators and CMV lysate (in CMV-reactive donors). This demonstrates that hyporesponsiveness of alloanergized PBMC is specific to FP alloantigens.
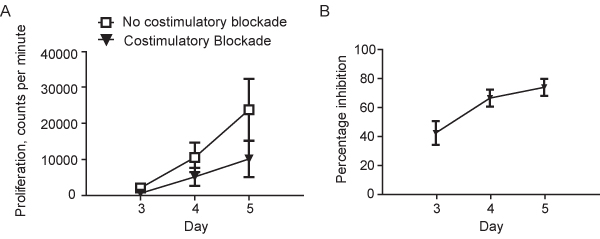
Figure 1. A.Proliferation (determined by thymidine incorporation) in a Primary Mixed Lymphocyte Reaction using HLA-mismatched stimulator and responder peripheral blood mononuclear cells (PBMC) in the absence or the presence of costimulatory blockade using humanized monoclonal anti-B7.1 and -B7.2 antibodies. Results are shown as mean (+/-sd) for 8 representative experiments using unique stimulator-responder pairs. B. Percentage inhibition of alloproliferation in primary MLRs performed in the presence of costimulatory blockade using humanized monoclonal anti-B7.1 and -B7.2 antibodies. Results are shown as mean (+/-sd) for the same 8 unique stimulator-responder pairs depicted in Figure 1A.
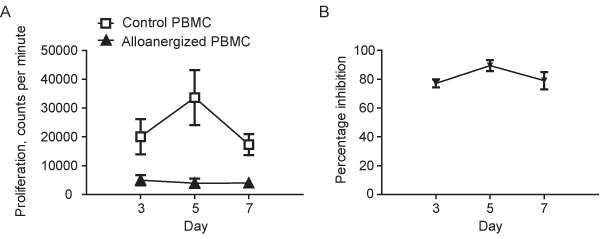
Figure 2. A. Proliferation (determined by thymidine incorporation) in secondary MLRs where responder PBMC from primary MLRs performed in the absence (control PBMC) or the presence of costimulatory blockade (alloanergized PBMC) are restimulated with irradiated first party stimulators. Results are shown as mean (+/-sd) for the 8 unique stimulator-responder pairs depicted in Figure 1. B. Percentage inhibition of First Party alloproliferation in secondary MLRs where responder PBMC from primary MLRs performed in the absence (control PBMC) or the presence of costimulatory blockade (alloanergized PBMC) are restimulated with irradiated first party stimulators. Results are shown as mean (+/-sd) for the 8 unique stimulator-responder pairs depicted in Figure 1 and Figure 2A.
