1. Preparation of Artificial Sputum Medium (ASM)
- Add 4 g DNA from fish sperm to 250 ml sterile water very slowly over a period of several hours. The DNA takes several hours to completely dissolve and can be stirred overnight at room temperature.
- Add 5 g mucin from porcine stomach (type II) slowly to 250 ml sterile water until the mucin has dissolved completely. The solution can be stirred overnight at 4 °C.
- Dissolve 0.25 g of each essential and non-essential L-amino acid, with the exception of L-tyrosine and L-cysteine, in 100 ml sterile water. Dissolve 0.25 g of L-cysteine in 25 ml of 0.5 M potassium hydroxide (Mr 56.11 g/mol) and 0.25 g of L-tyrosine in 25 ml sterile water.
- Dissolve 5.9 mg diethylenetriaminepentaacetic acid (DTPA), 5 g NaCl and 2.2 g of KCl in 100 ml of sterile water.
- Combine the DNA, Mucin, L-amino acids, DTPA, NaCl and KCl in a 1 litre bottle.
- Add 5 ml of egg yolk emulsion and fill to approximately 850 ml with sterile water.
- Adjust pH to 6.9 with 1 M Tris (pH 8.5; Mr 121.14) and bring the volume to 1 litre with sterile water.
- Sterilize the ASM by filtration using a Vacuubrand ME 2 diaphragm vacuum pump and Millipore Steritop filter units with a pore and neck size of 0.22 μm and 45 mm, respectively. Each Steritop filter unit can be re-used immediately up to three times; however, the filters need to be rinsed twice with sterile water before re-use. The filtration process is slow and can be performed over 2 days. Other versions of ASM have been developed that use the addition of antibiotics instead of filtration11 however, due to possible drug interactions, we do not recommend the method for this particular application.
- Unfiltered and filtered ASM should be stored at 4 °C in the dark. Using fresh ASM is recommended however, it can be kept under these conditions for a maximum of one month.
2. Determination of the Planktonic Sessile Cell Minimum Metabolic Inhibitory Concentration (PSMIC)
- To determine the minimum metabolic inhibitory concentration (PSMIC) values for 15 planktonically grown P. aeruginosa isolates, the microdilution method should be performed, as described in the guidelines of the British Society for Antimicrobial Chemotherapy BSAC12. The antibiotic of choice, in this case tobramycin sulphate, is serially diluted in Luria-Bertani (LB) medium in a 96-well microtitre plate to provide an appropriate range of antibiotic concentrations.
- Dilute overnight cultures of P. aeruginosa in LB to an OD600 of 0.05 (±0.01) and add 100 μl volumes to the wells of the 96-well microtitre plate containing 100 μl of the serially diluted antibiotic. In this case, the final concentrations of tobramycin sulphate ranged between 512 – 0.5 μg/ml. Eight replicates of each antibiotic concentration should be performed.
- Negative control wells for each isolate should be set up, in which no antibiotic is added. Also, eight wells should contain only LB for use as a blank during downstream analysis (Section 2.6).
- Incubate the 96-well microtitre plates for 1 – 2 days at 37 °C without shaking under aerobic or microaerophilic (5 % O2, 10 % CO2, and 85 % N2) conditions. Microaerophilic conditions are obtained using CampyGen gas generation packs in large anaerobic jars.
- Following incubation, bacterial growth is determined by measuring the absorbance of the bacterial culture in each well at a wavelength of 600 nm using a Fluostar Omega microplate reader and the MARS Data Analysis Software.
- Absorption from antibiotic-treated planktonic cultures (Aantibiotic treated planktonic cells) and absorption from the negative controls (Anegative control) should be corrected by subtraction of the background absorbance obtained from the wells containing LB only (Ablank). The percentage inhibition of viability is subsequently calculated as (mean Aantibiotic treated planktonic cells/mean Anegative control)x 100 %. The PSMIC90 is defined as the antibiotic concentration causing 90 % inhibition of planktonic bacterial growth.
- To determine bacterial viability after treatment with the antibiotic of choice, 10 μl of 0.02 % (v/v) resazurin (diluted in distilled water) is added to each well and the plates are incubated under aerobic conditions for 1 – 2 h at 37 °C, while shaking at 150 rpm. Viable cells will reduce the blue resazurin dye to the pink fluorescent resorufin form.
- Following incubation with resazurin, monitor the fluorescence of each well using an excitation wavelength of 540 nm and an emission wavelength of 590 nm in a Fluostar Omega microplate reader. The data should be analysed as described below.
3. Determination of Biofilm Sessile Cell Minimum Inhibitory Concentration (BSMIC)
- Overnight cultures of P. aeruginosa (in this case, 15 isolates of P. aeruginosa are used) should be diluted in LB to an OD600 of 0.05 (±0.01), then further diluted 1:100 in fresh ASM (total volume 1.8 ml).
- The diluted cultures (1.8 ml) should be added to each well of a 24-well tissue culture treated plate. Three wells should contain ASM only for use as a blank during downstream analysis (Section 3.9).
- Secure the 24-well plates with laboratory parafilm and incubate for 3 days under aerobic or microaerophilic conditions at 37 °C, while shaking at 75 rpm. Microaerophilic conditions should be obtained using CampyGen gas generation packs in large anaerobic jars.
- Dilute the antibiotic of choice, in this case tobramycin sulphate, to provide an appropriate concentration range in fresh ASM. In this instance, final concentrations ranged between 512 – 1 μg/ml. Add each concentration of the antibiotic, in volumes of 200 μl, to the appropriate wells of the 24-well plates. Four replicates of each antibiotic concentration should be performed. Biofilms not exposed to the antibiotic of choice were used as a negative control.
- Secure the 24-well plates with laboratory parafilm and incubate under aerobic or microaerophilic conditions for a further 24 h at 37 °C, while shaking at 75 rpm.
- After incubation in the presence of the antibiotic of choice, disrupt the bacterial biofilms using 100 μl of 100 mg/ml cellulase (diluted in 0.05 M citrate buffer [9.6 g/l Citrate.H20 in water and pH to 4.6 with NaOH]) and incubate the 24-well plates under aerobic conditions at 37 °C, while shaking at 150 rpm for 1 h. If required, biofilms could be further disrupted by manual pipetting at this stage.
- To determine the metabolic activities of the bacterial cells released from the disrupted biofilms, 100 μl of 0.02 % (v/v) resazurin (diluted in distilled water) should be added to each well of the 24-well plates and incubated for 1 – 2 h at 37 °C, while shaking at 150 rpm.
- Following incubation with resazurin, measure the fluorescence of each well using an excitation wavelength of 540 nm and an emission wavelength of 590 nm in a Fluostar Omega microplate reader and the MARS Data Analysis Software.
- Fluorescence from the antibiotic-treated biofilms (Fantibiotic-treated biofilms) and fluorescence from the negative controls (Fnegative control) should be corrected by subtraction of the background fluorescence obtained from the wells containing ASM only (Fblank). The percentage inhibition of viability is subsequently calculated as (mean of Fantibiotic treated biofilms/mean Fnegative control) x 100 %. The BSMIC90 is defined as the antibiotic concentration causing 90 % inhibition of metabolic activity.
4. Representative Results
ASM biofilm formation is possible in small (2 ml) volumes and the biofilms are fully formed within 3 days (Figure 1A). This can be demonstrated by rigorously pipetting the biofilm, which should be difficult to disrupt. The microcolonies are comparable to those grown in larger volumes4 (Figure 1B). Figure 2 shows major differences between cells grown planktonically and in a biofilm as detected by electron microscopic image analysis. Biofilm cultures clearly show considerable levels of extracellular matrix surrounding the cells and individual structures within the biofilm are difficult to identify.
Several studies suggest that the biofilm lifestyle can affect antimicrobial susceptibility13, 14. Our small scale ASM assay can be used to determine the BSMIC of multiple antibiotics for multiple isolates at the same time. The workflow of the assay is shown in Figure 3. The effect of antibiotics on bacterial cell viability can be measured using the resazurin assay. Antibiotics, in this case tobramycin, can be added to the established biofilm and incubated for 24 h. After this the biofilm is disrupted and resazurin is added.
Metabolically active cells can reduce the resazurin dye resulting in a colour change from blue (resazurin) to pink (resorufin) 15. Figure 4A shows an example assay in which P. aeruginosa was incubated with different concentrations of tobramycin before biofilm disruption and addition of resazurin in a microtitre plate. The blue non-fluorescent colour indicates non-viable cells, whereas viable cells reduce the dye to the pink fluorescent form, resorufin. The SMIC can then be calculated by converting fluorescence into percentage remaining bacterial viability. Figure 4B shows the change in % viability with increasing tobramycin concentration. 10% viability was chosen as a cut-off in order to calculate the SMIC90.
Under aerobic conditions, the tobramycin SMIC90 values are higher for cells grown as a biofilm than those of planktonic cultures. Table 1 shows the variation in PSMIC90 and BSMIC90 for all isolates tested. Table 2 shows that under aerobic conditions, a dramatic increase in resistance to tobramycin (2 to >32 fold increase in SMIC) was observed for most isolates when grown in ASM (biofilm mode) compared to LB (planktonic mode). In addition, biofilms grown under microaerophilic conditions exhibited an increased SMIC of between 2 and >128-fold when compared to biofilms grown under aerobic conditions.
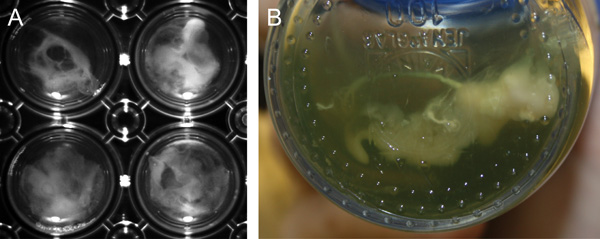
Figure 1. Biofilm formation of P. aeruginosa in ASM P. aeruginosa strain PAO1 forms macroscopically visible clumps (microcolonies) when grown in ASM. A, Biofilm formation in 30 ml ASM cultures (large-scale) after 7 days growth in screw cap glass Duran flasks . B, Biofilm formation in 2 ml ASM cultures (small-scale) after 3 days growth in 24-well polystyrene plates.
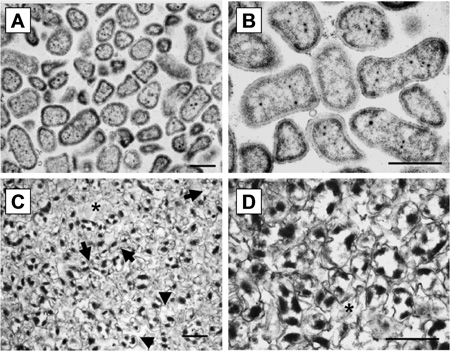
Figure 2. TEM micrographs of ASM biofilms A/C TEM micrograph (x;27,000) of PAO1 grown planktonically and in ASM, respectively, B/D TEM micrograph (x57,000) of PAO1grown planktonic and in ASM, respectively. Planktonically grown bacteria were cultivated overnight in LB broth. Biofilms were cultivated for 7 days in 30 ml ASM cultures. Black arrows refer to cells within the biofilm and stars refer to extracellular spaces. Scale bars = 1 μm.
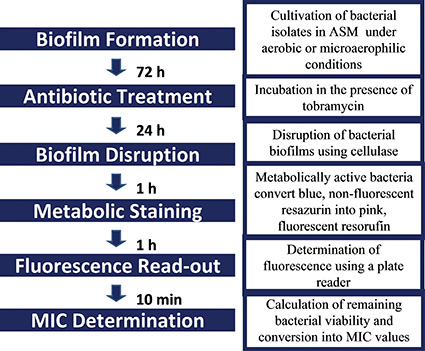
Figure 3. Workflow of the ASM biofilm antimicrobial susceptibility assay.
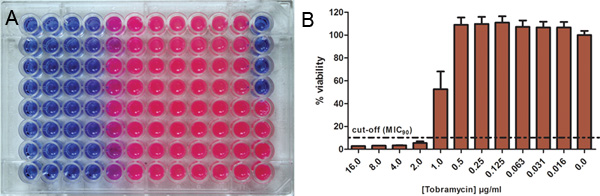
Figure 4. Use of resazurin for the determination of antibiotic susceptibilities Bacterial cells were incubated with different concentrations of the antibiotic and the remaining metabolic activity was determined using resazurin. A, The blue non-fluorescent oxidized form of resazurin indicates non-viable cells and is reduced by metabolic active cells to pink fluorescent resorufin. B, Fluorescence intensity is converted into percentage of remaining bacterial viability. 10% viability was chosen as cut-off in order to calculate the MSMIC90. Click here to view larger figure.
| Strains | PSMIC 90 (μg/ml) 1 | BSMIC 90 (μg/ml) 1 | ||
| Aerobic | Microaerophilic2 | Aerobic | Microaerophilic 2 | |
| PAO1 | 4 | 4 | 8 | >512 |
| Liverpool Epidemic Strain (LES) isolates | ||||
| LESB5821 | 8 | 64 | 64 | 128 |
| LES40022 | 32 | 128 | 8 | 256 |
| LESB25 | 16 | 32 | 256 | 512 |
| LESB55 | 16 | 64 | 64 | >512 |
| LESB64 | 16 | 64 | >512 | >512 |
| LES43122 | 4 | 8 | 32 | >512 |
| LESB49 | 16 | 64 | 64 | 256 |
| LES109 | 32 | 128 | 32 | >512 |
| Non-LES isolates | ||||
| 49461 | 16 | 32 | 16 | >512 |
| 59032 | 0.5 | 2 | 4 | >512 |
| 59073 | >512 | >512 | >512 | >512 |
| 59076 | 16 | 32 | 32 | >512 |
| 27 | 8 | 16 | 4 | >512 |
| 45 | 16 | 32 | 4 | >512 |
Table 1. Susceptibility of P. aeruginosa to tobramycin.
1For determination of PSMICs and BSMICs tobramycin was used in 2-fold serial dilutions
ranging from 512 – 0.5 μg/ml (n = 8 for each concentration) and 512 – 1 μg/ml (n = 4 for each
concentration), respectively;; PSMICs were determined using the standard
microdilution method1.
2Microaerophilic conditions were 5 % O2, 10 % CO2, and 85 % N2.
| Strain | PSMIC90/BSMIC90fold change1 | |||
| PSMICaerobic → PSMICmicroaerophilic |
BSMICaerobic → BSMICmicroaerophilic |
PSMICaerobic → BSMICaerobic |
PSMICmicroaerophilic → BSMICmicroaerophilic |
|
| PAO1 | 0 | >64 | 2 | 128 |
| LES isolates | ||||
| LESB58 | 8 | 2 | 8 | 2 |
| LES400 | 4 | 32 | 0.25 | 2 |
| LESB25 | 2 | 2 | 16 | 16 |
| LESB55 | 4 | >8 | 4 | >8 |
| LESB64 | 4 | ND | >32 | >8 |
| LES431 | 2 | >16 | 8 | >64 |
| LESB49 | 4 | 4 | 4 | 4 |
| LES109 | 4 | 16 | 0 | >4 |
| Non-LES isolates | ||||
| 49461 | 2 | >32 | 0 | >16 |
| 59032 | 4 | >128 | 8 | >256 |
| 59073 | ND | ND | ND | ND |
| 59076 | 2 | >16 | 2 | >16 |
| 27 | 2 | >128 | 0.5 | >32 |
| 45 | 2 | >128 | 0.25 | >16 |
Table 2. Fold change of PSMICs and BSMICs to tobramycin.
1ND, not determined; values in bold indicate SMIC fold changes >10.
