On unenhanced images, the synovium of infected knees presents a diffuse swelling of intermediate signal that is non distinguishable from surrounding soft tissue, while femur and patella appear as low signal structures (Figure 1).
On the USPIO-enhanced images, 24 hr after the contrast agent administration, synovial area containing USPIO-loaded macrophages will demonstrate signal loss (Figures 1 and 2).
Macrophage infiltration within synovium can be demonstrated using specific immunostaining (Figure 3). Perls' Prussian blue stain can detect iron particles, which appear as blue dots (Figure 4).
| GRE T2 weighted | |
| Repetition time (msec) | 450 |
| Echo time (msec) | 4 |
| Flip angle | 30 |
| Turbo factor | |
| Fat suppression | |
| Slice thickness (mm) | 1.5 |
| Interval gap | 0 |
| Field of view (mm) | 70 |
| Matrix | 448 x 360 |
| Bandwidth | 80 |
| Signals acquired | 2 |
| Scan length | 3'10 |
Table 1. Example of parameters of GRE T2-weighted MR sequence on a 3T MR unit.
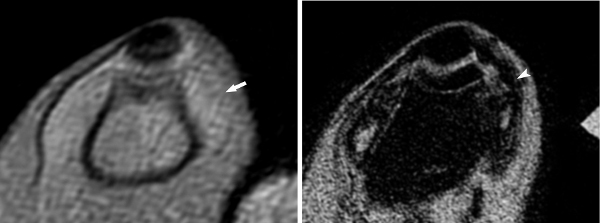
Figure 1. Axial GRE T2-weighted images of a rabbit knee at the acute phase of infection, before (A) and 24 hr after (B) intravascular administration of the USPIO; Images are obtained at the level of the patella (p) and femur (f). On the unenhanced image (A), the synovium is thickened (arrow) and presents a homogenous intermediate signal indistinct from the surrounding soft tissues. After USPIO administration (B), the synovium appears now as a band-like area of massively dark signal (arrowhead) due to the presence of USPIO-loaded macrophages. (reprinted from Lefévre S. et al.9 with permission).
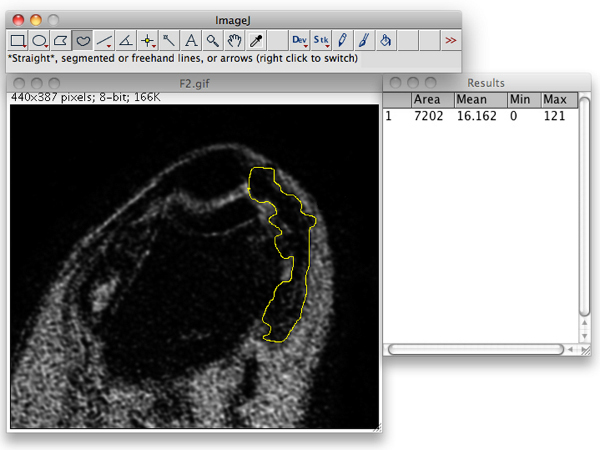
Figure 2. Segmentation and determination of the synovial area that presented signal loss using ImageJ.
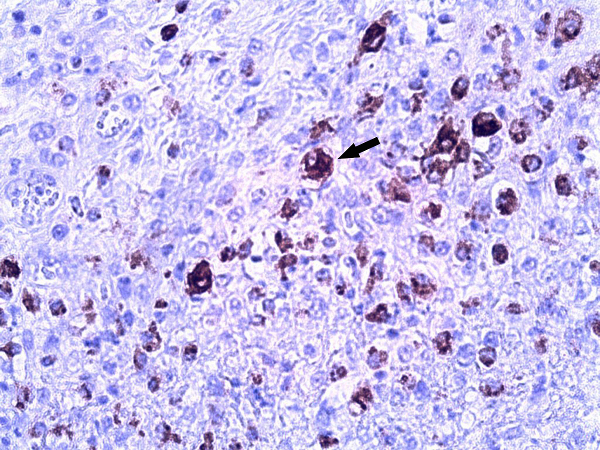
Figure 3. Photomicrograph of specific macrophage immunostaining demonstrates the intense infiltration of macrophages within the infected synovium (arrow). (RAM 11 immunostaining, original magnification 40X).
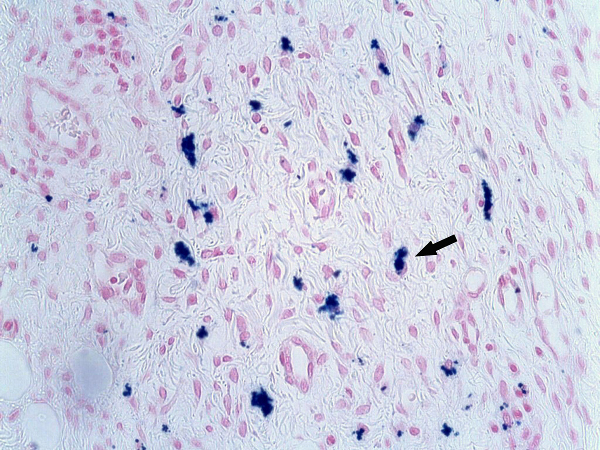
Figure 4. Photomicrograph (Perls' Prussian blue stain, original magnification 40X) shows multiple blue-stained cells correspondig to the USPIO-loaded macrophages (arrow). (Reprinted from Lefévre S. et al.9 with permission).
