One hundred outpatient HIV-1-infected persons were prospectively tested for clinical markers of frailty to include shrinking weight, slowness in walking, decrease in grip strength, low activity, and exhaustion. Eighty-one patients were not frail when studied, 19 patients were frail at the initial assessment (Table 1). The characteristics of the frail and non-frail patients were not significantly different except for a higher rate of hepatitis C and neuropathy in the frail group (p < 0.05). Length of infection with HIV, CD4 count and HIV-1 RNA viral load were also compared. As shown in Table 2 the younger patients had a greater incidence of frailty and this was associated with low CD4 cell counts. CD4 counts <200 cells/mm3 were associated with 9-fold increased odds of frailty relative to patients with a CD4 count >350 cells/mm3 (odds ratio [OR] 9.0, 95% confidence interval [CI] 2.1-44). Seven frail patients were measured 6 months later: 2 died refusing therapy, 4 were no longer frail, and 1 patient remained frail (Table 3). From this data it appears that when patients took prescribed anti-retroviral therapy the CD4 cell counts improved along with an improvement in the general state of health of the patient. Finally, if the incidence of frailty in the study population is compared to the number of years of anti-retroviral therapy taken by the patients, the longer patients took anti-retroviral therapy, the less the incidence of frailty (p < 0.05). This fact supports the early use of anti-retroviral therapy in HIV-infected patients which is the preferred approach in recent HIV treatment guidelines.15
We conclude that frailty is common in HIV outpatients and is associated with low CD4 counts more than with advancing age. Our data suggest that frailty is transient, especially in younger patients who may revert to their prefrail state unlike uninfected elderly individuals in whom a stepwise decline in function may occur.
Representative Results from our Previous Study1
| Frail, N=19 (19%) | Non-Frail, N=81 (81%) | ||
| Sex | Male | 14 (74%) | 60 (74%) |
| Female | 5 (26%) | 21 (26%) | |
| Age | <50 | 12 (63%) | 46 (57%) |
| >=50 | 7 (37%) | 35 (43%) | |
| Comorbidity | Dyslipidemia | 6 (32%) | 25 (31%) |
| Psychiatric | 4 (21%) | 29 (36%) | |
| Neuropathy | 8 (42%) | 15 (19%) | |
| Hypertension | 2 (11%) | 17 (21%) | |
| Hepatitis C | 6 (32%) | 12 (15%) | |
| Diabetes mellitus | 3 (16%) | 6 (7%) | |
| Coronary artery disease | 1 (1%) | 5 (6%) |
Table 1. Clinical characteristics of the HIV study patients. Frail patients were compared to non-frail HIV patients with respect to sex, age and comorbidities. The presence of neuropathy and infection with hepatitis C were significant differences between the frail and non-frail patients.
| CD4 Cell Count (cells/μl) | <50 Years of Age, N (%) | >=50 Years of Age, N (%) |
| <200 | 7 | 3 |
| 200-350 | 4 | 1 |
| >350 | 1 | 3 |
| Ρ-value | 0.028 | 0.021 |
Table 2. Frail patients and the relationship of age and CD4 cell count in these patients. The frail patients were significantly younger and with lower CD4 cell counts than non-frail patients.
| Patient | Initial CD4 Cell Count (cells/μl) | Initial Viral Load (RNA copies/μl) | Retest CD4 Cell Count (cells/μl) | Retest Viral Load (RNA copies/μl) | Comorbidity | Outcome |
| 1 | 26 | 2 million | N/A | N/A | hepatitis C, alcoholism | Dead; refused ART |
| 2 | 3 | 52,000 | 1 | 82,000 | coccidioido-mycosis | Dead; stopped ART |
| 3 | 12 | 12,000 | 36 | <48 | none | Not frail |
| 4 | 169 | <48 | 991 | <48 | blindness, peripheral neuropathy, pulmonary embolism | Not frail |
| 5 | 141 | 1,000 | 54 | <48 | lymphoma, peripheral neuropathy | Not frail |
| 6 | 151 | <48 | 393 | <48 | coccidioido-mycosis, deep venous thrombosis | Not frail |
| 7 | 106 | 44,620 | 229 | <48 | hepatitis C, chronic obstructive lung disease | Frail |
Table 3. Outcomes of 7 frail patients with low CD4 cell counts. These patients all needed anti-retroviral therapy, were prescribed therapy and then retested for frailty 6 months later. Only one patient who took the prescribed anti-retroviral therapy was still frail 6 months later.
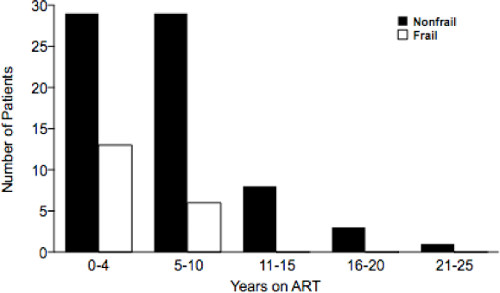
Figure 1. Relationship between number of years of taking anti-retroviral therapy and the incidence of frailty (89 patients were taking anti-retroviral therapy). The longer patients took anti-retroviral therapy the less the incidence of frailty in that population (p < 0.05).
